About Us
We would like to welcome you to the web-site of Campaign for ME Clinics Worldwide.
There are over 20 million people suffering from ME around the world. The complexity of ME, Fibromyalgia and Chronic Lyme disease requires specialist medical doctors with a high level of training, experience and knowledge. The experience in other countries, especially from private clinics, shows that specialist ME clinics, Fibromyalgia clinics and Chronic Lyme disease clinics are the most effective and cost efficient means of treating these complex diseases. We aim to get governments, foundations, philantrophies, private organisations, investors, etc. together to fund the building of ME clinics in countries all over the world.
We are coordinating our efforts with the National Institutes of Health (NIH) in the USA and working with them to develop new research approaches, new biological diagnostics and treatments, and new medical clinics based on the findings of scientific research and the clinical data of medical doctors and specialist medical clinics. One of our members regularly attends NIH meetings. Our efforts are ongoing.
What is ME ? Have People died from ME and its health complications ?
M.E. stands for Myalgic Encephalomyelitis which is a Latin name meaning inflammation of the brain, spinal cord and muscles. Myalgic Encephalomyelitis or ME was first used to define the illness by Dr. Donald Acheson in the Lancet medical journal in 1955 and has been used ever since - Outbreak at the Royal Free.
E.D Acheson. The Lancet, Volume 266, Issue 6886, Pages 394 - 395, 20 August 1955. ME is the correct scientific and medical name for the illness. The World Health Organisation (WHO) classification code for ME is G93.3, World Health Organisation - Classification . This is universally accepted by governments, medical associations and doctors worldwide. This classifies ME as a neurological illness, and puts ME in the same class as other neurological illnesses such as Multiple Sclerosis, Parkinsons, ALS, Epilepsy.
Dr. Melvin Ramsay, a British medical doctor was a leading global authority on ME from 1955 to 1990, and his work was cited and used by doctors around the world. Dr. Melvin Ramsay was a consultant physician at the Infectious Diseases Department of the Royal Free Hospital, and he also served as advisor to the British Ministry of Health in matters concerning smallpox. He was actively involved in treating ME patients during the famous Royal Free Hospital outbreak in England. In 1956, a paper by Dr. Melvin Ramsay appeared in the Lancet Encephalomyelitis simulating Poliomyelitis He believed that there was an infectious cause which led to neurological, endocrine, mitochondria and muscular abnormalities. His research paper 'Epidemic neuromyasthenia' 1955-1978'. Postgrad Med J. 1978 Nov;54(637):718-21. PMID:
746017, was a major contribution to medicine, and provided important insights into the illness in Britain over 2 decades. His classic book about ME, detailing its naming, definition and it's progression through the 1950's, 1960's and 1970's is Myalgic Encephalomyelitis and Post Viral Fatigue States: the Saga of the Royal Free Disease by Dr Melvin Ramsay. A later paper in 1990, co-authored by Dr. Ramsay provided new and deeper insights into ME Myalgic encephalomyelitis--a persistent enteroviral infection?. Dr. Ramsay knew and collaborated with other ME experts such as Dr. Acheson and Dr. Richardson throughout this period and their medical and scientific insights were very valuable and continue to have relevance today. Dr. Ramsay was the first person to create a formal definition and diagnostic criteria for the illness in 1986, which was used by doctors and researchers in Europe - Ramsey ME Definition 1986, 1988 . This defintion and diagnosis is still relevant today.
Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. His work corroborated and verified the medical and scientific findings of Dr. Melvin Ramsay (mentioned above). He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME. These medical and scientific findings are still important and are the subject of ongoing scientific research.
The scientific research into ME much of it catalogued below and in the Scientific Evidence Section, confirms that ME is a multi-factor neurological illness with chronic infection, immune dysfunctions, endocrine abnormalities, mitochondria dysfunctions and destruction, exertion intolerance, heart and vascular abnormalities, sleep cycle abnormalities. These chronic infections and biological dysfunctions remain undiagnosed for many years and decades due to old, primitive and outdated diagnostic methods and technologies. ME is a severe disability and can last for years and decades, and has led to many premature deaths from medical neglect. If carefully diagnosed and treated, using modern advanced diagnostic technologies and methods, it can over several months and years be reduced in its effects, and in some cases patients restored back to normal health, and most importantly lives saved. The most effective medical diagnostics and treatments and medical clinics are listed on this web site.
It should be emphasised again that many thousands of patients have died from this illness, especially in epidemics. ME type epidemics prior to 1955, are listed in the section ME Epidemics below. They date back to 1917, but there is a general medical and scientific consensus that the illness itself is far older, as epidemics in the past would would not have been identified and defined due to primitive medical knowledge and techniques, and totally inadequate medical technologies. Medical doctors were unable to properly diagnose and treat patients, and many became severely disabled or died. A mixture of arrogance and ignorance held back medical progress. Past epidemics would have used several terms to define the illness, examples being ‘Epidemic Neuromyasthenia’, 'Atypical Poliomyelitis’, 'Iceland disease', ‘Encephalitis’, 'Encephalitis lethargica', Neurasthenia', ‘Akureyri Disease’, ‘Poliomyelitis-like epidemic neuromyasthenia’, 'Diencephalitis', ‘Abortive Poliomyelitis’. The link to chronic enterovirus infection is obvious from the names given to it throughout history. These are mentioned in the following research papers:
After 1955, Dr. Acheson's paper which named and described the ME illness, was followed by an article in the Lancet by Sigurdsson describing the illness and it's history A new Clinical Entity ? in 1956. In that same year, a paper by Dr. Melvin Ramsay appeared in the Lancet Encephalomyelitis simulating Poliomyelitis . Dr. Melvin Ramsay was a consultant physician at the Infectious Diseases Department of the Royal Free Hospital, and he also served as advisor to the Ministry of Health in matters concerning smallpox. He was actively involved in treating ME patients during the Royal Free Hospital outbreak. He went on to become a leading global expert in ME, spending 35 years diagnosing, treating and researching ME, and other diseases. There was another paper by Dr. Acheson in the Lancet in 1957 Benign myalgic encephalomyelitis followed by an article in the British Medical Journal titled 'Epidemic Myalgic Encephalomyelitis' in 1957. The ME outbreak at the Royal Free Hospital in Britain continued to interest doctors and researchers as evidenced by the paper An Outbreak of Encephalomyelitis in the Royal Free Hospital Group, London, in 1955 by THE MEDICAL STAFF OF THE ROYAL FREEHOSPITAL in British Medical Journal in 1957.And another paper that year Epidemiological aspects of an outbreak of encephalomyelitis at the Royal Free Hospital, London, in the summer of 1955
In 1957, a paper by an American, Dr. Shelokov , 'Epidemic Neuromyasthenia. An outbreak of poliomyelitis-like illness in student nurses' published in the New England Journal of Medicine provided details of a typical ME outbreak, which was quite new to medical science in America. That year a paper was published in the New England Journal of Medicine about the Punta Gorda outbreak. Another paper in 1958 shed more light on the illness - Benign myalgic encephalomyelitis. Galpine, J.F. Brit. J. Clin. Practice, 12:
186, 1958. This was followed by another more detailed paper by Dr. Acheson in the American Journal of Medicine in 1959, The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromyasthenia.n 1959 a paper appeared in the New England Journal of Medicine titled 'Epidemic Neuromyasthenia — Clinical Syndrome?' by Dr. Donald Henderson and Dr. Shelokov and this gave an an American perspective on the disease, ME. In 1955, Pellew and Miles (1955) in Australia reported that the infectious agent in ME patients was transferred to healthy monkeys and they died within a short time. Autopsies showed damage to nerve cells and blood vessels. A medical thesis by Dr. A.L. Wallis in Edinburgh University, 1957 shed some light on the outbreak of ME in Cumberland in the 1950's. An autopsy of a dead patient showed damage to nerve cells and blood vessels. The common consensus among doctors and researchers during the 1950's was that a virus was involved. By 1960, 'Myalgic Encephalomyelitis' (ME) was formally accepted and recognised by medical authorities worldwide, and in 1962 it began appearing in medical text books in University. Dr. Donald Acheson was convinced the illness involved a chronic infection with neurological, muscular and immunological effects and dysfunctions. Dr. Acheson later became the Chief Medical Officer in Britain and was a highly respected medical doctor and researcher.
There were further research papers and reviews produced by other leading medical doctors and researchers including Dr. Melvin Ramsay, Dr. E. O'Sullivan, Dr. Richardson, Dr. Galpin, Dr. Deisher, Dr. Parish, Dr. Shelokov, Dr. Henderson, Dr. Sigurdsson, Dr. Poskanzer, Dr. Gsell, Dr. Hill, Dr. Dowsett, Dr. Behan and others in medical and scientific journals throughout the 1950's, 1960's, 1970's and 1980's, see History of ME presented by Lisa Petrison to the CFSAC in 2014. They all concluded that an infectious disease, neurological dysfunctions, musco-skeletal dysfunctions, exhausation, mitochondria abnormalities, and severe inflammation were involved in the illness.
It's neurological aspects were considered important by the medical community, and ME was formally classified by the World Health Organisation as a neurological disorder in the International Classification of Diseases (ICD) in 1969 (ICD-8: Vol I: code 323, page 158; Vol II (Code Index) page 173).
Dr. Erich Ryll a US doctor based in California studied ME patients from 1975 to 1994. He concluded that it involved infectious vasculitis, extreme inflammation, severe exhausation, and that an infectious disease was involved. Vasculitis involving the skin was recorded during ME outbreaks in Cumberland, Durham and North West London in Britian in 1955. This has been confirmed by later studies showing significant vascular abnormalities and damage to veins in ME patients.
ME Epidemics and Pandemics throughout History There have been well documented ME epidemics, pandemics, and outbreaks throughout history. These include the following:
1917 Van Economo reports an illness involving brain and neurological inflammation, weakness, and great fatigue and some deaths. See paper 'New Clinical Entity' published in the Lancet in 1956.
1918 - 1924, several outbreaks of an illness involving brain and neurological inflammation, weakness, and severe fatigue reported throughout Europe. See paper 'New Clinical Entity' published in the Lancet in 1956.
1924 England and Wales 5,039 cases of encephalitis lethargica. See paper 'New Clinical Entity' published in the Lancet in 1956.
1934
Los Angeles County Hospital. Called 'Atypical Poliomyelitis'
1936
Fond Du Lac, Wisconsin - St. Agnes Convent - Encephalitis
1937
Erstfeld, Switzerland -
Abortive Poliomyelitis
1937
St. Gallen, Switzerland
- Frohburg Hospital – Abortive Poliomyelitis
1939
Middlesex, England - Harefield Sanatorium
1939
Degersheim, Switzerland - Abortive Poliomyelitis
1945
Pennsylvania. Hospital of the University of Pennsylvania - epidemic Pleurodynia
1946
Iceland
disease resembling Poliomyelitis with the character of Akureyri disease
1948
Iceland, North Coast towns - epidemic simulating Poliomyelitis
The outbreak in Iceland was important, and provided some vital clues about the illness.
"However,
children
in epidemic Neuromyasthenia areas
responded
to
poliomyelitis
vaccination
with
higher
antibody titres
than
in
other
areas
not
affected
by
the
poliomyelitis
epidemic,
as
if
these
children
had
already
been
exposed
to
an
agent
immunologically
similar
to
poliomyelitis
virus
(Sigurdsson,
Gudnad6ttir Petursson,
1958).
Thus,
the
agent
responsible
for
epidemic Neuromyasthenia would
appear
to
be
able
to
inhibit
the
pathological
effects
of
poliomyelitis
infection.
When
an
American
airman
was
affected
in
the
1955
epidemic
and
returned
home,
a
similar
secondary
epidemic
occurred
in
Pittsfield,
Massachusetts,
U.S.A.
(Hart,
1969:
Henderson
and
Shelokov,
1959)."
Many outbreaks of ME or epidemic Neuromyasthenia worldwide followed an outbreak of polio virus.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
1948 300
sporadic
cases
of
epidemic Neuromyasthenia
seen
in
South
California
between
1948
and
1965.
1949
Adelaide, South Australia - a disease resembling Poliomyelitis
1949 Cambridgeshire, England -
aberrant poliomyelitis. Involvement of other Enteroviruses suspected.
1950
Louisville, Kentucky -- St. Joseph
's Infirmary - epidemic Neuromyasthenia
1950
Upper State New York -- outbreak resembling the
Iceland disease, simulating
"
acute Anterior Poliomyelitis
1952
London, England - Middlesex Hospital Nurses
'
Home - Encephalomyelitis
associated with Poliomyelitis virus
1952
Copenhagen, Denmark - epidemic Myositis
1952
Lakeland, Florida - epidemic Neuromyasthenia
1953
Coventry and District, England - an illness resembling Poliomyelitis observed in
nurses
1953
Rockville, Maryland - Chestnut Lodge Hospital - Poliomyelitis-like epidemic
Neuromyasthenia
1953
Jutland, Denmark - epidemic Encephalitis with vertigo
1954 Tallahassee, Florida - epidemic Neuromyasthenia
1954 Seward, Alaska - benign Myalgic Encephalomyelitis (Iceland Disease)
1954
Berlin, Germany - British army - further outbreak of a disease resembling
Poliomyelitis
1954
Liverpool, England - outbreak among medical and nursing staff in a local
hospital
1954 Johannesburg,
South
Africa - epidemic Neuromyasthenia
1955
Dalston, Cumbria, England – epidemic and sporadic outbreak of an unusual
disease
1955
London, England - Royal Free Hospital - outbreak in staff and patients of Benign
Myalgic Encephalomyelitis
1955 Hampstead, London
1955
Perth, Australia - virus epidemic in waves
1955
Gilfac Goch, Wales - outbreak of benign Myalgic Encephalomyelitis
1955
Durban City, South Africa - Addington Hospital. Outbreak among nurses called 'Durban Mystery Disease' also called 'epidemic Neuromyasthenia'
1955
Segbwema, Sierra Leone - outbreak of Encephalomyelitis
1955
Patreksfjorour and Porshofn, Iceland - unusual response to polio vaccine
1955
Northwest London, England - nurses
'
residential home - acute Infective
Encephalomyelitis simulating poliomyelitis
1956
Ridgefield, Connecticut - epidemic Neuromyasthenia
1956
Punta Gorda Florida - outbreak of epidemic Neuromyasthenia
1956
Newton-le-Willows, Lancashire, England - Lymphocytic Meningoencephalitis with
myalgia and rash
1956
Pittsfield and Williamstown, Massachusetts - benign Myalgic Encephalomyelitis
1956
Coventry, England - epidemic malaise, benign Myalgic Encephalomyelitis
1957
Brighton, South Australia - Cocksakie Echo virus Meningitis, epidemic Myalgic
Encephalomyelitis
1958
Athens, Greece - nurses
'
school - outbreak of benign Myalgic Encephalomyelitis
with periostitis and arthopathy noted.
1958
Southwest London, England - reports of sporadic cases of Myalgic
Encephalomyelitis
1959
Newcastle Upon Tyne, England - outbreak of benign Myalgic Encephalomyelitis
1961
Basel, Switzerland - sporadic cases of benign Myalgic Encephalomyelitis
1961
New York State - outbreak of epidemic Neuromyasthenia in a convent
1964
Northwest London, England - epidemic malaise, epidemic Neuromyasthenia
1964
Franklin, Kentucky - outbreak of Neuromyasthenia in a factory
1965 Lamarque,
Texas,
U.S.A.
- epidemic Neuromyasthenia. Investigated by Leon-Sotomayor
(1969).
1967
Edinburgh, Scotland - sporadic cases resembling benign Myalgic
Encephalomyelitis
1968
"
Fraidek, Lebanon - benign Myalgic Encephalomyelitis
1969
Brooklyn, New York - State University of New York Downstate Medical Center -
epidemic Neuromyasthenia, unidentified symptom complex
1970
Lackland Air Force Base, Texas - epidemic Neuromyasthenia
1970
London, England - Great Ormond Street Hospital for Children - outbreak of
Neuromyasthenia among nurses
1975
Sacramento, California - Mercy San Juan Hospital - Infectious Venulitis, epidemic
"
Phelobodynia
1976
Southwest Ireland - epidemic Neuromyasthenia, benign Myalgic
Encephalomyelitis
1977
Dallas – Fort Worth, Texas - epidemic Neuromyasthenia
1979
Southampton, England - Myalgic Encephalomyelitis
1980
West Kilbridge, Ayrshire, Scotland - epidemic Myalgic Encephalomyelitis
1980
San Francisco, California – epidemic persistent flu-like illness
1981
Stirlingshire, Scotland
- sporadic Myalgic Encephalomyelitis
1982
West Otago, Dunedin and Hamilton, New Zealand - Myalgic Encephalomyelitis
1983
Los Angeles, California - initial cases of an unknown, chronic symptom complex
involving profound "fatigue"
1984
Lake Tahoe Area of California/Nevada - start of a yearlong epidemic involving
"
over 160 cases of chronic illness eventually characterized as Chronic Fatigue
Syndrome Source: Paradigm Change web site
The Invention of the name 'Chronic Fatigue Syndrome' or CFS and the False Diagnosis of CFS In the USA, the name M.E. was used from the 1950's to 1988. Many American scientific researchers and doctors used the term ME to describe the illness in their papers and publications. Medical Journals in Europe and North America used the term ME. In 1985, there was an ME type epidemic in the Lake Tahoe area in the USA. Then in 1988, something bizarre happened, this ME illness and ME epidemic in Lake Tahoe was given the name 'Chronic Fatigue Syndrome (CFS)' by the CDC. Though at the CDC meeting, there were sharp divisions between older, experienced medical doctors, such as Hyde, Parish and Shelokov, who had studied ME for decades and wanted to continue using the existing term 'ME' to name and describe the illness, and a new NIH administrator called Stephen Straus who wanted to invent a new name for the illness calling it 'Chronic Fatigue Syndrome'. After some heated rows, arguments and disputes, Hyde, Parish and Shelokov left the CDC group. Straus fraudulently succeeded in giving ME a new name calling it "Chronic Fatigue Syndrome", which proved to be disastrous for patients, doctors and scientific researchers. The new name has proved very insulting to patients and very ambiguous, vague, and confusing for medical doctors and scientific researchers. This is discussed in more detail in sections below and includes, facts, letters and correspondence.
Central to this new, ineffective and confusing name 'Chronic Fatigue Syndrome' (CFS) are the Lake Tahoe medical and scientific findings which point to chronic immune system dysfunctions, chronic viral infection(s), chronic inflammation, muscular abnormalities, exertion intolerance, and some neurological and endocrine dysfunctions, all of which are found in ME epidemics. It was a typical ME epidemic. Straus chose to ignore this and the facts, medical and scientific evidence from previous ME epidemics. Calling ME by another name has confused and divided medical opinion and scientific opinion ever since. Would one call Diabetes "Chronic Thirst Syndrome" or call Cancer "Chronic Weakness and Pain syndrome" or call Alzheimers disease "Chronic Forgetting Syndrome" or call Parkinsons disease "Chronic Tremor Syndrome" or call Anemia "Chronic Tiredness Syndrome" ?? The answer would be 'no' as they are insulting, abusive and tell one nothing about the illness. Then why did Mr. Straus use an insulting and abusive term such as "Chronic Fatigue Syndrome" to describe an ME type illness, an ME epdemic?
There is evidence that Mr. Straus (NIH) acted maliciously to make the illness "evaporate" and disappear and become a non illness - click here to view letter exchanged between Dr. Straus and Dr. Fukuda shortly after the Fukuda definition was approved in 1994. He deliberately worked with others to omit the scientific and medical evidence, give the illness a bad name and a poor quality definition, belittle and denigrate it, deprive it of legitmacy and of research funding, and make the illness disappear. The illness did not disappear. In fact it continued to increase with outbreaks occurring during the 1990's and into the 21st century. These actions by Straus contributed to the medical neglect of patients, mockery of the illness, no research funding, no attempt to replicate biological findings and identify biomarkers and to the deaths of tens of thousands of patients worldwide. This was serious medical misconduct. This was also accompanied by fraud, criminal behaviour and deceit by certain government bodies in the USA, which is discussed in sections below. Dr. Byron Hyde, a top expert in ME provides an insight into ME and the medical and financial scandals involved.
In 2015, the prestigious Institute of Medicine and the American National Academy of Science published their medical and scientific findings about ME in a book "Beyond ME". This was the result of 2 years of research, including a review of 2,700 scientific research papers and expert testimonies by medical doctors and scientists by a 15 strong medical committee. They renamed the illness Systemic Exertion Intolerance Disease (SEID), and stated that: "the term 'chronic fatigue syndrome' can result in stigmatization and trivialization and should no longer be used as the name of this illness." Finally the fraud committed by Straus had been exposed, dismissed and replaced with a more scientific name.
CFS is a term invented in 1988 and is a false diagnosis. It diagnoses nothing and explains nothing and is useless. Many doctors no longer use the term 'CFS' or 'Chronic Fatigue Syndrome'.
WHO Classification
ME is the correct scientific and medical name for the illness. The World Health Organisation (WHO) classification code for ME is G93.3, World Health Organisation - Classification . This is universally accepted by governments, medical associations and doctors worldwide. This puts ME in the same class as other neurological illnesses such as Multiple Sclerosis, Parkinsons, ALS, Epilepsy.
The research verifies that it is a neurological illness with immune deficiencies, endocrine abnormalities, mitochondria dysfunctions, and chronic infections in most cases.
Medical Diagnostic Protocols and Treatment Protocols using Best International Practices
ME is a chronic physical illness, which is multi-factorial, involving immune system dysfunctions, neurological dysfunctions and abnormalities, chronic infections of the nervous system, brain, muscles, glands and intestines in subgroups of patients, HPA axis and endocrine dysfunctions, mitochondria abnormalities and dysfunctions and cardiac and vascular system abnormalities. Some doctors and scientific researchers believe that ME has a long history and they cite previous names for ME such as ‘Epidemic Neuromyasthenia’, 'Atypical Poliomyelitis’, 'Iceland disease', ‘Encephalitis’, 'Encephalitis lethargica', ‘Akureyri Disease’, ‘Poliomyelitis-like epidemic neuromyasthenia’, 'Diencephalitis', ‘Abortive Poliomyelitis’. Fibromyalgia is common in both ME and Chronic Lyme patients, and has it's own biological markers. There is international agreement between experienced doctors, scientific researchers, medical authorities and governments in relation to what constitutes ME.
What is ME ? Summary of Scientific Research Findings
Primary biological dysfunctions and abnormalities
(1) ATP, Mitochondria & Krebs cycle dysfunctions, including destruction of Mitochondria
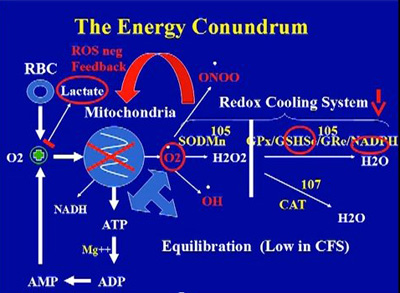
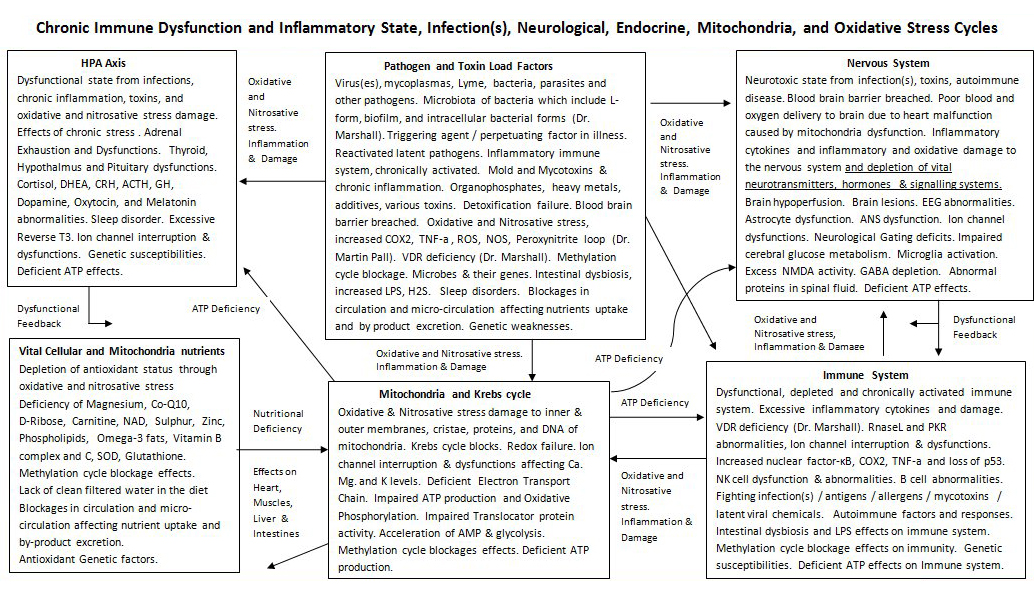
The research and clinical work of Dr. Sarah Myhill, Dr. Behan and Dr. Paul Cheney and other doctors and researchers have consistently found this biological abnormality. Deficient ATP produced and deficient recycling of ATP. A rapid shift to anerobic metabolism, build up of lactic acid, purines, muscle pains etc. during and after exercise, and post-exercise malaise commonly found in ME patients. Oxidative & Nitrosative stress damage to inner & outer membranes of mitochondria, cristae, proteins, and DNA of mitochondria. Krebs cycle blocks. Redox failure. Ion channel interruption & dysfunctions affecting Ca. Mg. and K levels. Deficient Electron Transport Chain. Impaired ATP production and Oxidative Phosphorylation. Impaired Translocator protein activity. Acceleration of AMP & glycolysis. This may be due to chronic infections, a chronically activated inflammatory immune system, hypoxia or lack of oxygen in cells, toxins and the high levels of oxidative and nitrosative stress in the illness. It is known by scientists that some viruses such as EBV, other herpes viruses and retroviruses and bacteria such as mycoplasma and Borrelia (Lyme disease) can interfere with, disrupt and destroy the mitochondria. These infections are regularly found in ME and CFS patients.
Mitochondria dysfunction and destruction is the most important factor as the mitochondria and krebs cycle produces ATP, which is fuel or energy for the immune system, the nervous system, the brain, the muscles, the heart, the glands, and all the organs. Any significant deficiency in ATP will cause a slow down in the activity of these organs and the body, and more serious deficiencies can cause extreme tiredness and fatigue most or all of the time. This mitochondria damage over time may also explain Cardiac dysfunctions in ME.
(2) Immune system dysfunctions and deficiencies caused by or accompanied by viral / mycoplasma / pathogen infection (active and latent) and/or toxins. Overactive 2'-5' oligosynthetase pathway, defects in the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway with effects on immune system function and important ion channels. In the case of the 2-5a synthetase / RnaseL anti-viral pathway, it is believed that human leukocyte elastase and/or calpain cleaves the 80 kDa form of RnaseL into 37 kDa RnaseL, cleaves STAT1-alpha protein and p53 protein and Actin, bringing about deficiencies in these proteins. These proteins are essential for normal immune system function, and their depletion and abscence leads to serious and continuing immune system dysfunction. These abnormalities strongly indicate an immune system which is being activated by chronic viral infection, and the immune system is becoming depleted or defective over time.
There is an accompanying increase in NF-Kb levels and activity which is pro-inflammatory. Low numbers of NK cells and reduced NK cell function and cytotoxicity. The Rituximab studies show that B cell abnormalities, including excessive levels of defective B cells are a major factor and may perpetuate the illness. Scientists such as Pender and others believe that chronic EBV infection of B cells plays a role in ME, CFS and other autoimmune illnesses. Chronic immune system activation with dominance of pro-inflammatory cytokines. T cell abnormalities, including depleted Suppressor cells, CD8 and T reg cell abnormalities and an abnormal CD4/CD8 ratio. Retrovirus infections have been found in ME patients, and these infections can deplete T cell suppressor cells and other T cell subsets. Interferon poisoning in some subgroups of patients, and this is is also linked to viral infections. The overactive immune system is progressing to autoimmunity in some cases, there are HLA abnormalities and other evidence of autoimmunity in many patients. VDR abnormalities which weaken immunity, and increase susceptibility to chronic infection and autoimmune risk (Dr. Marshall, Marshall Protocol). Gastrointestinal abnormalities which contribute to immune system dysfunctions.
The immune system has a high demand for ATP in this illness, while ATP is being depleted through mitochondria destruction or degradation.
(3) the evidence from prior ME epidemics show that infections play a role in most ME patients. Top ME doctors A. Gilliam, Melvin Ramsay, Elizabeth Dowsett, John Richardson of Newcastle-upon-Tyne, W.H. Lyle, Elizabeth Bell, James Mowbray of St Mary’s, Peter Behan and Byron Hyde all believed that the majority of primary M.E. patients fell ill following exposure to an Enterovirus. Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME. Historically, Enterovirus infections mainly target the nervous system, brain, muscles and intestines, all of which abnormal in ME patients.
In subgroups, there is evidence of Retrovirus infection and Herpes infections and changes to cell structures and to T cell subsets. There is evidence for continuing viral, mycoplasma, bacteria and other pathogen infections (both active and latent, including partially latent) of the nervous system, nerve junctions, brain, immune system cells, intestines, joints, muscles, and other body organs. These infections may be causative, opportunistic or a co-factor in the illness. There are high levels of oxidative and nitrosative stress and inflammation, and cellular destruction, arising from chronic immune system activation, infections, immune system and cellular dysfunctions, and toxins.
Secondary
biological dysfunctions and abnormalities (1) dysfunctions of the central nervous system, the brain and the autonomic nervous system, and involves significant chronic inflammation, lesions, reductions in grey and white matter, brain hypoperfusion, increased ventricular lactate, spinal fluid abnormalities, autonomic dysfunctions and other abnormalities. This adversely affects many other body functions.
(2) Dr. Paul Cheney has found toxic build up in the body in many patients. Flow reversal in the liver and the brain. Chronic Cerbral Spinal Venous Insufficiency (CCSVI). Chronic He patic Venous Insufficiency (CHVI). Cardiac Dysfunction. This reversal leads to auto-intoxication and a build up of toxins and toxin related damage to cells, tissues, organs, glands, etc.. (Dr. Paul Cheney) (3) methylation cycle blocks and glutathione deficiency. The methylation cycle is important and produces many substrates and co-factors for other body organs and processes, including the mitochondria. Deficient glutathione increases oxidative and nitrosative stress and this contributes to mitochondria abnormalities and dysfunctions. (4) HPA axis dysfunctions, in particular hypothalmus gland, adrenal gland and thyroid gland dysfunctions and abnormal hormone output, which adversely affects hormones, sleep and immune function.
All of these 7 factors are the core of the illness, the perpetuating factors over time. Subgroups will contain most of the 7 factors mentioned above. There are slight differences between patient groups which are due to subgroups, genetic differences, different environment exposures and toxins, different infectious agents, different microbiome and metagenome status, and different diet and lifestyles. These abnormalities and dysfunctions have a domino effect on other cellular functions and body functions leading on to several other dysfunctions, and to severe illness.
The immune system dysfunctions and abnormalities in ME patients makes them more susceptible to various infections. The acquired infection(s) will depend on one's geographical location and exposures, and one's genetic status and immune system status. Some of the following pathogens have been consistently found in ME patients:
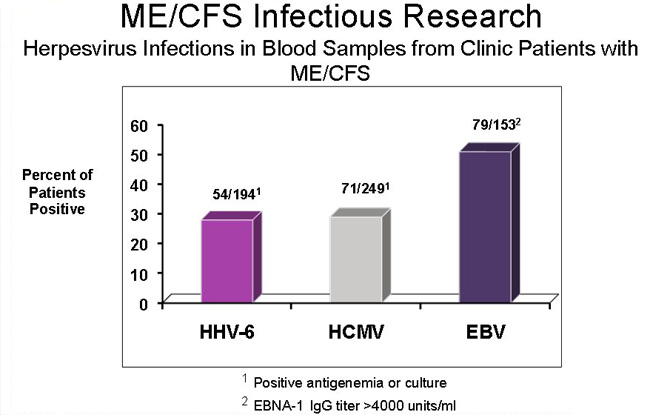
Viruses include: Reactivated (latent) EBV virus, particularly in B cells, nervous system, glands and organs, HHV6a virus, Herpes family viruses 1-8, CMV, Coxsackie viruses, Enteroviruses, Polio type viruses, Parvovirus B-19,Ross river virus, Q fever virus, Stealth virus, JHK virus, Parainfluenza Virus-5 (PIV-5), Paramyxovirus and measles viruses of the Paramyxoviridae family, Cryptovirus, Borna virus, HTLV family viruses, HGRV virus in spinal fluids, nerve tissues, blood, brain, intestines, and muscles. Retroviruses are important, as Retrovirus sequences were found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in Columbia University in September 2013. Most of these viruses listed here would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Reactivated latent viruses include EBV, HERV-K18, Varicella-Zoster virus, Herpes family viruses 1-8, Enteroviruses, Polio type viruses, measles viruses of the Paramyxoviridae family. Some viral infections can reactivate latent viruses and undermine immune system functions.
Co-Factors in ME
Mycoplasma: M. fermentans, M. penumoniae, M. hominis, M. penetrans, M. pirum, M. incognito. in intestines, spinal fluids, blood, brain, nerve tissues, muscles. These mycoplasmas would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Bacteria: Chronic Lyme disease, Ehrlichia, Bartonella, Brucella, Rickettsia, Chlamydia pneumonia, Staphylococcus spp. (live blood analysis), and Bacteria, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms in spinal fluids, intestines, blood, brain, nerve tissues, muscles. Intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism (Dr. Kenny De Meirleir). These bacteria would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Parasite: Cryptostrongylus pulmoni (rare cases), Babesia, Candida, Giardia lamblia, Aspergillus Niger Molds, Bacteria and Mycotoxins in water damaged buildings: Stachybotrys family of molds, Cladosporium, Penicillium, Alternaria, Aspergillus, mycobacteria, Actinomycetes, Lipopolysaccharides (LPS), Microbial Volatile Organic Compounds (VOCs), Hemolysins.
These can cause chronic inflammatory immune response and immune dysfunction over time.
These infections may be causative, opportunistic or a co-factor in the illness.
Most patients are infected with EBV and suffered mononucleosis at some stage in their life. Over 90% of adults carry one or more herpes viruses for life. Latent infections can last a human lifetime (80 -100 years). EBV goes into a latent stage after active infection, and tends to live inside B cells. It can also live in other body organs. EBV uses the machinery of the B cells to replicate itself and to migrate to other body parts. The infected and abnormal B cells is a key factor in this illness. These deep infections of immune cells and body organs along with molecular mimicry can create conditons of autoimmunity which are directly related to the site of EBV infection. Chronic EBV infection and other Herpes infection or latent incubation in the liver, the spleen, the thyroid gland, the joints, adrenal glands and the nervous system can lead to variety of autoimmune conditions, which can confuse doctors.
EBV (and other Herpes viruses) may be able to undermine the effectiveness of CD8 T cells and NK cells and the TH1 cytokine system, which are the body's main defence against viruses and bacteria. These immune deficiencies are regularly found in ME and other autoimmune illnesses.
Rituximab, B-cell abnormalities & Viral induced Autoimmunity & Cancers
The scientific findings show that B-cell abnormalities play a significant role in autoimmunity in ME, and the success of the drug Rituximab confirms these findings. The scientific research of Fluge and Mella in Norway show that depleting B-cells through Rituximab brings about recoveries in two thirds of patients. Yet this takes several months to achieve. Once Rituximab is withdrawn, the patients become ill again after a few months, as B-cell numbers increase. Viruses / mycoplasmas may be hiding in B-cells so as to infect patients and/or increasing B-cell production for infection purposes, indirectly causing both an autoimmune response and an ongoing infection. Dr. Martin Lerner (Michigan, USA) believes that anti-virals kill the viruses, but do not hit the B-cells which incubate the virus(es) and that Rituximab hits the B-cells, but has little effect on the viruses. This would explain why Rituximab improves ME patients after a few months, but when Rituximab is stopped, the patients deteriorate, as (infected) B cell populations increase again. Dr. Michael Pender in his paper CD8+ T-Cell Deficiency, Epstein-Barr Virus Infection, Vitamin D Deficiency, and Steps to Autoimmunity: A Unifying Hypothesis. Pender MP. Autoimmune Dis. 2012;2012:189096. postulates that EBV virus is capable of living inside B cells and using the machinery of these cells to replicate itself, and cause continuing infection, autoimmunity and immune dysfunction which could last for years and decades. He also states that reduced cytotoxic T cell function plays a key role in this, allowing EBV infection of B cells and other cells to continue. This is explored further in the following papers Could the Epstein-Barr Virus – Autoimmunity Hypothesis Help Explain Chronic Fatigue Syndrome ? and EBV I: A Deficient Immune Response, Increased Levels of Epstein-Barr Virus Opens Up EBV Question in Chronic Fatigue Syndrome Again. An excellent scientific paper produced by scientific researchers in Germany in 2014 shows the importance of chronic EBV infection, including persistent reactivation of latent EBV combined with a defective immune system. This plays a major role in ME (Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome.
Loebel M, Strohschein K, Giannini C, Koelsch U, Bauer S, Doebis C, Thomas S, Unterwalder N, von Baehr V, Reinke P, Knops M, Hanitsch LG, Meisel C, Volk HD, Scheibenbogen. Scientific analysis and discussion on http://simmaronresearch.com/2014/03/1591/ )
Listing of Research findings and papers worldwideand categorisation of biological abnormalities and dysfunctions and infections found in ME
The following paper by the organisation Paradigm Change details many of the biological abnormalities, dysfunctions and infections found in ME and CFS patients and research papers to support this. ME and Medical Abnormalities - Medical Research paper.
The Dubbo Studies which were published in leading medical journals verify much of the above, and point to genetic factors, environmental factors and a post-infectious dysfunctional immune system as being the key factors in ME .
Serious Illness and Deaths
The potent combination of immune dysfunction and multiple infections, mitochondria and Krebs cycle malfunction, Neurological dysfunctions, Cardiac, Endocrine and HPA axis dysfunction cause a patient to become very exhausted and weak over time. Many ME sufferers end up bed-ridden, house bound or in wheelchairs. ME can be deadly, thousands of people around the world have died of ME and health complications caused by ME , see Memorial section. New research into causes of death in ME presents a very disturbing picture, click here to view findings
Comedians like Ricky Gervais have made fun of and mocked and laughed at such disabled people, and this is despicable, perverted, ignorant and disgraceful behaviour by him. Ricky Gervais should educate himself about illnesses before mocking them. If his wife, children, or mother and father were dying of this illness, he would have behaved differently. Unfortunately societies and people are becoming dumbed down, and ignorance and stupidity accepted as "normal". There should be standards, ethics and laws in the entertainment industry to strongly discourage and punish such behaviour.
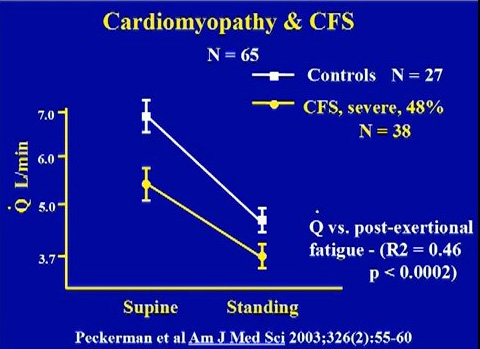
ME bears a resemblance to Cancer and AIDS in the sense that many ME patients have died of opportunistic infections, heart failure and certain cancers due to a depleted immune system and high levels of oxidative stress (and it's effects). Research has recently shown that most ME patients have serious heart and vascular abnormalities arising from ME , making them highly susceptible to a sudden heart attack. ME patients have died prematurely of heart attacks, and this is a continuing and worrying pattern of the illness. There is also a high rate of suicide among ME patients, this being brought about by frustration, desperation for some cure, social isolation, lack of support, constant pain, exhaustion and weakness, and financial hardships.
On 15th October 2009, Professor Nancy Klimas, then Professor of Medicine, Microbiology and Immunology at the University of Miami, famously said in the New York Times: “I hope you are not saying that ME patients are not as ill as HIV patients. I split my clinical time between the two illnesses, and I can tell you that if I had to choose between the two illnesses I would rather have HIV”. Dr. Nancy Klimas, is an internationally respected doctor and Immunologist and an expert in both ME and AIDS.
"There is evidence that the patients with this illness experience a level of disability that is equal to
that of patients wi
th late
-
stage AIDS, patients undergoing chemotherapy (and) patients with
multiple sclerosis" Professor Nancy Klimas, University of Miami, speaking at the launch of the US
CDC campaign to raise awareness of ME, 3 November 2006, National Press Club, Wa
shington
DC
In 1995, Professor Mark Loveless, Head of the AIDS and ME Clinic at Oregon Health Sciences University said in his US Congressional Briefing that an ME patient: “feels effectively the same every day as an AIDS patient feels two weeks before death; the only difference is that the symptoms can go on for never-ending decades”. Mr. Loveless supported his statement with data from research conducted at his own institution and morididity data provided by other ME experts who had compared the two diseases (AIDS and ME ).
In 1994, Dr. Anthony Komaroff of Harvard Medical School reported that the brains of those people with ME were identical to those with AIDS dementia, when viewed with SPECT imaging. They were both completely different to normal healthy brains. He believed that ME cases were the result of viral infection of the brain and nervous system, similar to AIDS.
SPECT imaging of the brain: comparison of findings in patients with chronic fatigue syndrome, AIDS dementia complex, and major unipolar depression.
Schwartz R , Komaroff AL, Garada BM, Gleit M, Doolittle TH, Bates DW, Vasile RG, Holman BL. AJR Am J Roentgenol. 1994 Apr;162(4):943-51.
"There is no question in my mind that this is a physical disorder. The fact that we haven‘t been smart enough or invested enough in it to sort that, doesn’t mean that this is anything else." Professor Dr. Ian Lipkin, Columbia University. He is internationally recognized as an authority on the use of molecular methods for pathogen discovery. Dr. Lipkin has over 30 years of experience in diagnostics, microbial discovery and outbreak response, has mentored and trained more than 30 students and post-doctoral fellows and leads a team of over 65 investigators, post-doctoral fellows and research and support staff in New York City and another 150 across the world. https://www.mailman.columbia.edu/people/our-faculty/wil2001
In September 2012, Dr Sandra Kweder of the FDA in America called ME "a serious or life threatening disease".
In 1994, one of the world’s most renowned ME clinicians, Dr Daniel L Peterson from the US, went on record: “In my experience, it is one of the most disabling diseases that I care for, far exceeding HIV disease except for the terminal stages” (Introduction to Research and Clinical Conference, Fort Lauderdale, Florida, October 1994; published in JCFS 1995:1:3-4:123-125).
In 2004, Dr William Reeves, Chief of the ME research programme at the US Centres for Disease Control, (CDC) reported that ME patients “are more sick and have greater disability than patients with chronic obstructive lung or cardiac disease, and that psychological factors played no role” (Press Release, AACFS, 7th October 2004).
Also in 2004, a randomised clinical trial found “In comparison with other chronic illnesses such as multiple sclerosis, end-stage renal disease and heart disease, patients with ME show markedly higher levels of disability” (Am J Occup Ther 2004:58:35-43).
In 1990, Dr. Nancy Klimas published a research paper in the Journal of Clinical Microbiology, in it she reported that the array of immunological defects in ME suggests that it is a form of acquired immuno-deficiency (Nancy Klimas, et al "Immunologic abnormalities in Chronic Fatigue Syndrome", Journal of Clinical Microbiology, 28, (June 1990)
Dr. Paul Cheney (who has successfully treated hundreds of ME patients) stated "These patients look a lot more like multiple sclerosis (MS) patients or AIDS dementia patients, whose dysfunctions are also subcortical".
On the Sickness Impact Profile Scale (SIPS), ME patients test as high or higher than people with Cancer and heart attack (Oslers Web, by Hillary Johnson, Penguin Books 1997, page 292).
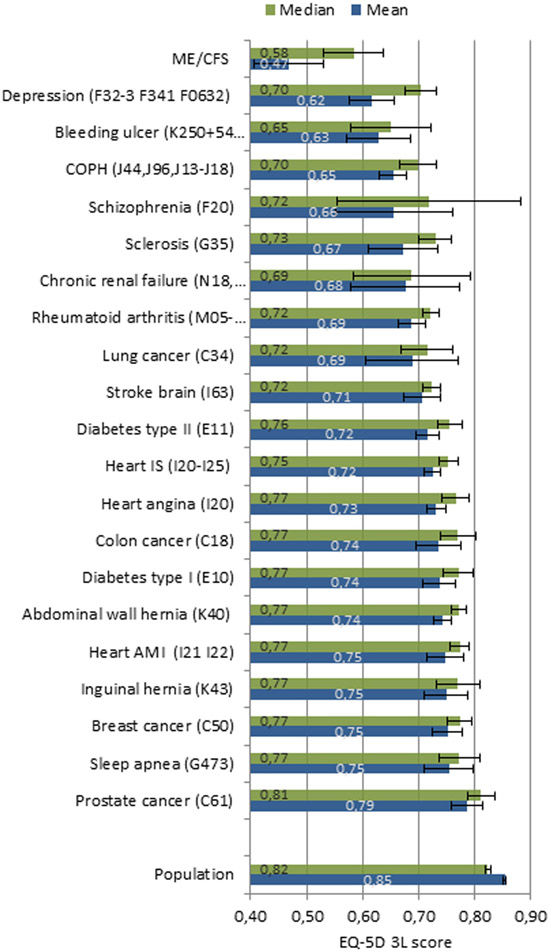
According to research in 2015, Quality of Life measurements for ME patients were lower than those suffering Cancers, Depression Rheumatoid Arthritis, Schizophrnia, diabetes, heart diseases. See the chart below. The lower quality of life for ME patients is a major contributing factors to the high rate of suicide for ME patients.
The following Facebook message and petition by an ME advocate outlines the problem faced by many patients, particularly severe ME cases
ill ME patient being
taken to hospital.
The Documentary 'I Rememeber ME' provides a very emotional account of the effects of ME on individuals, families and communities across the USA. The failures of government and the Federal health bodies are very apparent. It can be viewed on the following link - http://www.youtube.com/watch?v=401--WCB5dc
Another documentary film shows the effects of severe ME. More information about this documentary can be found at http://www.methehiddentruth.com/
Response of some Governments
The fact that patients are dying of this illness while other patients are disabled for many years and decades, and that this imposes massive costs on the economy, means that governments should act to implement clinics, hospital departments and new diagnostic labs to properly diagnose and treat this illness. A few governments are taking this illness seriously. Several other governments have been asked to take action but refused, with some citing that bailing out corrupt bankers and speculators using billions of euros (and dollars) of taxpayers money was their top priority and only priority.
We have listed the positive and constructive actions of some governments below:
In 2011, the Norwegian Government apologised to ME patients and their families in Norway for neglecting them, and offering ineffective, useless psychiatric and psychological treatments for many years, which left them sick and in limbo. The government announced a change in direction towards biological based diagnostics and treatments and support for biological research such as the Rituximab trials in Norway. Norway's Directorate of Health Apologises for Treatment of ME Patients
In 2001, Health Canada appointed an international panel of experts in this emerging field of medicine, ME , to establish a clinical working-case definition, diagnostic guidelines, and treatment procedures. The panel released a set of guidelines in 2003 and their choice of name to describe the condition was both "myalgic encephalomyelitis" and "chronic fatigue syndrome" – with acronyms shortening it down to a manageable size: ME. This document was legally commissioned and approved by Health Canada. This is a legally enforceable document in relation to patient's rights. It can be enforced through a Canadian court. Many medical doctors now use the Canadian Consensus criteria (2003) to diagnose and treat patients in Canada. See documents below Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols, 2003
and For Medical Doctors - Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Diagnostic and Treatment Protocols, 2003 for doctors and specialists in Canada.
The Swedish government have funded two small ME clinics in Sweden. These use the Canadian criteria and the ICC criteria.
- Gottfries clinic. Government funded from 1998 to 2017. Private clinic from January 2017 to present. Operates on the site of a government funded University.
- Stora Sköndal receives local government funding.
There is a high demand for their medical services. Most patients are satisfied with the quality of specialist medical care.
The Australian government also recommends use of the Canadia Consensus criteria (2003). This is outlined in the following Australian government web site http://sacfs.asn.au/download/guidelines.pdf
In Japan the Japanese Ministry of Health commissioned and approved a new definition in 2004 called 'Childhood Chronic Fatigue Syndrome', this detailed several immunological, neurological, sleep disorders,. endocrine, infectious factors in the illness. Childhood chronic fatigue syndrome. Miike T. Nihon Rinsho. 2007 Jun;65(6):1099-104.
In 2008, the Japanese Association of Fatigue Science which works closely with the Japanese Ministry of Health, published its definition, and diagnostic and treatment criteria for ME . Leading Japanese researchers and doctors were involved in this. It's defintion included immune system, neurological, endocrine and infectious factors. It was similar to the Canadian Consensus criteria (2003) and the later International Consensus criteria (2011). Though, the Japanese definition goes into a bit more detail. The Japanese Ministry of Health funds scientific research into the factors defined by the Japanese Association of Fatigue Science in their definition. Their defintion is being used in Japan at present. See papers below: Chronic Fatigue Syndrome Hirohiko Kuratsune,
Yasuyoshi Watanabe.
Fatigue Science for Human Health
2008, pp 67-88
Position paper - http://www.med.or.jp/english/pdf/2006_01/019_026.pdf
In Japan there is also a condition called called "Low natural killer cell syndrome" which is very similar to ME. Natural killer cell abnormalities are one of the most consistent findings in ME. The following papers outline the Japanese position on the illness. They correlate to some points in the aforementioned diagnostic criteria used by the Canadian and Norwegian governments.
- Aoki T, Usada Y, Miyakoshi H: A novel immunodeficiency: Low NK syndrome (LNKS). Jap J Med 3212:14-17, 1985
- Aoki T, Usuda Y, Miyakashi H, et al: Low natural syndrome: clinical and immunologic features. Nat Immun Cell Growth Regul 6:116-128, 1987
- Aoki T, Miyakoshi H, and Usada Y et al: Low NK syndrome and its relationship to chronic fatigue syndrome. Clin Immunol Immunopathol. 69:253-65, 1993.
The clinical features of low natural cell numbers, function and cytotoxicity is specific to ME and ME like Illnesses and "Low natural killer cell syndrome"
The diagnostic criteria used by the Canadian, Australian and Norwegian governments and health authorities represent best international practises and the latest medical and scientific research findings. They also integrate the 'Low natural killer cell syndrome' findings used by the Japanese government into their criteria.
Introductory Lectures by Medical Doctors and Scientists
Paper by Dr. Anthony Komaroff, Professor of Medicine at Harvard Medical School in the USA.He has been treating ME patients and researching the illness since 1987. He is an internationally recognised ME expert. He has advised several Federal Bodies in the USA on the subject of ME over the years.
Research findings by Dr. Ronald W Davis, a top scientist in the USA and Professor at Stanford University. He is working with a few Nobel Prize winners at the Open Medicine Foundation ( www.openmedicinefoundation.org ) to discover the biological causes and pathology of ME , it's diagnostics and treatments.
Dr. Kenny De Meirleir is medical doctor based in Belgium and in Nevada in the USA. He runs a well known medical clinic in Belgium and also works for the Whittemore Peterson Institute in Nevada in the USA. He has been treating ME patients and researching the illness since 1990. He has seen thousands of ME patients over the years. The medical and scientific findings of Dr. Kenny De Meirleir over 20 years support the role of infections and immune system abnormalities in ME . Lecture series by Dr. Kenny De Meirleir videos 1 - 20, created in 2012 and 2013. Specifically for medical doctors and hospital consultants and scientific researchers.
The film 'Unbroken' which is a major success in North America and Europe was based on a book written by Laura Hillenbrand who has ME (CFS). It depicts an American hero, Louis Zamperini, who overcame great adversity prior to and during world war 2.
Louis Zamperini read Laura Hillenbrand's other book 'A Sudden Illness' and he was deeply impressed by her courage in fighting the illness ME (CFS). He was so impressed by her bravery that he gave her his own Purple Heart medal which he won in the second world war. I have attached the letter with Purple Heart medal. The Purple Heart is only given for acts of great bravery which also involve personal injury in the act. Today Laura Hillenbrand owns this Purple Heart medal, to show great courage in the face of a terrible and painful illness, ME (CFS), and a determination to overcome and defeat this illness.
CBS news interviewed Laura Hillenbrand below. She explains her illness and what she has endured over 3 decades.
Dr. Byron Hyde is a medical doctor based in Canada. He has been treating ME patients and researching the illness since 1986, and he has seen thousands of ME patients. Dr. Hyde is an internationally recognised ME expert and has contributed much to research, and clinical practise methodologies, including the Canadian Consensus Criteria 2003 and International Consensus Criteria 2011. The following video lecture by him provides an overview of the problem of misdiagnosis. His medical textbook (below) for ME and provides an in-depth account of the problems of misdiagnosis and missed diagnoses. It also reveals innovative medical methods for properly diagnosing and treating the illness
Lecture on ME by Dr. Byron Hyde, Winter 2012
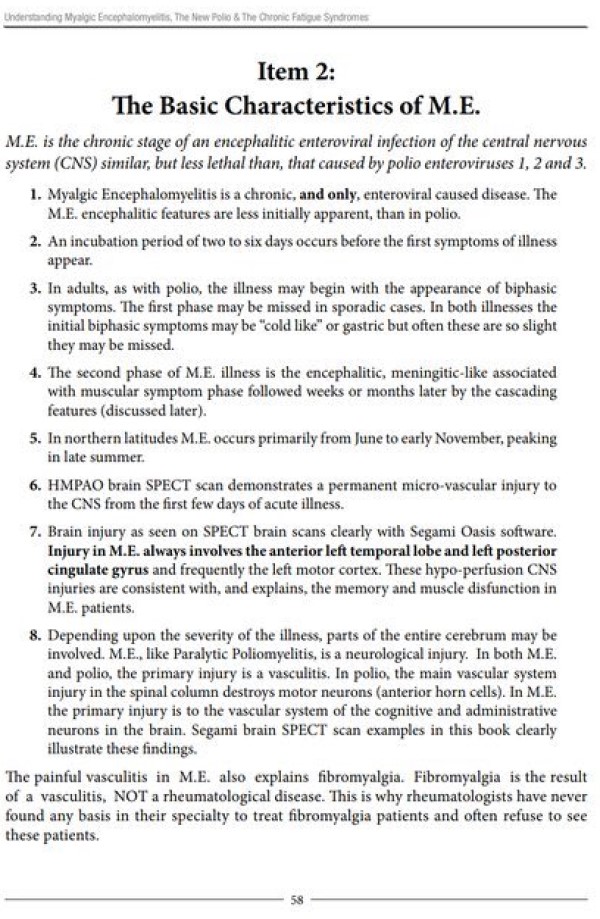
Source: Understanding Myalgic Encephalomyelitis : the New Polio and Chronic Fatigue Syndromes, Dr. Byron Hyde, Page 58
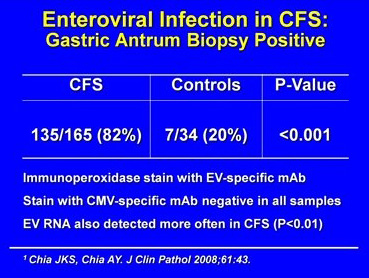
Enteroviruses are implicated accordign to Dr. Byron Hyde and other medical experts (See work of Dr. Chia below). This would include ECHO viruses, Enterovirus 71, and Coxsackie viruses. This would be high priority as a result of the historical association between ME and Enteroviruses in North America and Europe. The intestines, muscles and nerves being major reservoirs of infection. Dr. Chia in California has developed highly accurate tests. Test nervous system, brain, muscles, intestines, glands, blood, joints, heart and blood vessels.
It is important to note that some ME sufferers have been diagnosed properly using modern and accurate diagnostic criteria and many have not been diagnosed due to lack of knowledge of the illness and / or poor diagnostic methods and equipment in their state / country. It is estimated that 50% or more of people with ME have been undiagnosed with the illness and suffer from an illness they are unaware of. As more modern and accurate diagnostic criteria become accepted by governments and medical authorities, and diagnostic tests and equipment become more advanced and accurate and as doctors become more educated about this illness and specialist clinics become operational, and public awareness of the illness increases, there will be an increase in the number of people diagnosed with this illness. Applying this 1% finding to the global population would suggest that 70,000,000 people have this illness. Though global regional differences may exist due to varying toxic exposures, pathogen exposures, allergen exposures, lifestyle stress factors, pollution of foods, liquids and air, and other illness initiating factors. Population prevalance is discussed in more detail in the 'Why set up a Clinic' section on this web site.
The Views and Lectures by Leading Medical Doctors in the Field
Professor Anthony Komaroff M.D. of Harvard Medical School
has recently written the following:
(1) many patients with ME have no diagnosable psychiatric disorder and that ME is not a form of depression;
(2) there is a state of chronic, low-grade immune activation, with evidence of activated T cells and evidence of genes reflecting immune activation, as well as evidence of increased levels of cytokines;
(3) there is substantial evidence of poorly-functioning NK cells (white blood cells that are important in fighting viral infections);
(4) there is evidence of white and grey matter abnormalities in the brain;
(5) there is evidence of abnormalities in brain metabolism (and evidence of dysfunction of energy metabolism in the mitochondria);
(6) there is evidence of abnormalities in the neuroendocrine system, particularly in the HPA axis but also in the hypothalamic-prolactin axis and in the hypothalamic-growth hormone axis;
(7) there is evidence of cognitive difficulties, especially with information processing, memory and/or attention;
(8) there is evidence of abnormalities in the autonomic nervous system (including a failure to maintain blood pressure, abnormal responses of the heart rate, and unusual pooling of blood in the legs, as well as low levels of blood volume);
(9) there is evidence of disordered gene expression, especially in those genes that are important in energy metabolism and in genes connected to HPA axis activity, to the sympathetic nervous system and to the immune system;
(10) there is evidence of frequent infection with viruses, especially herpesvirus and enteroviruses.
Source: Summer 2008 issue of The CFIDS Chronicle published by The CFIDS Association of America.
Lecture by Dr. Dan Peterson providing a medical and scientific overview of ME (Stockholm, November 2011). Dr. Dan Peterson, a medical doctor has been treating ME patients since the mid 1980's and is an internationally acclaimed ME doctor and expert. (4 continuous videos of his lecture below)
Dr Harvey Alter, who discovered the hepatitis C virus, and works in the US National Institutes of Health (one of the top research institutes in the world) said in 2010: “I’m absolutely convinced that when you define this disease by proper criteria, this is a very serious and significant medical disease, and not a psychological disease. It has the characteristics of a viral disease”
Professor Luc Montagnier (who won the Nobel prize for discovering the AIDS virus) said: “Scientists have already uncovered a lot about ME, but this information does not reach professional healthcare personnel, and the disease is not taken seriously. It is about time this changes”
Understanding the Confusion in the Field - Names and Definitions and the Role of Arrogance and Ignorance 'Remember in describing the Lake Tahoe epidemic
this (Holmes) committee were describing a typical Myalgic Encephalomyelitis Epidemic.'
Source:
A Brief History of Myalgic Encephalomyelitis, by Dr. Byron Hyde
ME is often called CFS or Chronic Fatigue Syndrome. The term 'Chronic Fatigue Syndrome' was invented by Mr. Stephen Straus of the NIH in 1987 to describe an ME type illness and recent ME type epidemic in Lake Tahoe. He presumed to call ME another name such as 'Chronic Fatigue Syndrome'. Prior to 1987 there was no such thing as 'Chronic Fatigue Syndrome' or CFS. In 1987 and 1988, the CDC came under great pressure to investigate this ME type epidemic, which they did. The findings of medical doctors from Lake Tahoe were presented to the CDC at the time, and the CDC also carried out an investigation and gathered it's own data, and all of these findings (by doctors and the CDC) were published in scientific papers at the time. According to doctors and scientists, the Lake Tahoe epidemic had all the characteristics of an ME epidemic. Though some researchers and doctors called it Chronic Epstein Barr virus Syndrome (CEBV) at the time. This term became obsolete as a minority of patients had active EBV or reactivated EBV and some had other viruses and pathogens and immune system deficiencies.
In 1988, the Holmes committee of the CDC met to define the illness, but it became bitterly divided over what to call this illness, some favoured the medical term Myalgic Encephalomyelitis (ME) as it had most of the characteristics of this illness, while others disagreed. If the Lake Tahoe epidemic had occurred in Britain, the term Myalgic Encephalomyelitis (ME) would have been used, as evidenced by past epidemics and outbreaks there. But, Dr. Straus favoured the term he himself recently invented 'Chronic Fatigue Syndrome', and a definition which was loose and ambiguous, and he managed to manipulate a few others on the committee to support him. Some doctors, including Dr. Parish, Dy. Hyde and Dr. Shelokov disagreed with Straus and quit the CDC committee and refused to sign off on the final name and definition. Straus chose unwisely to ignore previous ME epidemics and his ignorance of these caused him to give ME a new name 'Chronic Fatigue Syndrome' which was both useless and ineffective from a medical and scientific perspective. Thus the very term or name 'Chronic Fatigue Syndrome' emerged from a mixture of ignorance and arrogance on the part of Straus and those naieve enough to follow him. Other factors also played a part in the CDC's final decision to label it 'Chronic Fatigue Syndrome', this included intense lobbying and pressure on national and state politicians by business owners in the Lake Tahoe area and Nevada state who wished to have this illness disappear or be labelled a non illness ; this is discussed in the book A Brief History of Myalgic Encephalomyelitis, by Dr. Byron Hyde. Business interests played a key role in this, yet ironically the families of some business owners later became ill with CFS, and suffered the consequences of this ill defined name and definition.
Dr. Byron Hyde's book, A Brief History of Myalgic Encephalomyelitis , details the activities of the Holmes Committee, and how it came to invent the term 'Chronic Fatigue Syndrome'. He also mentions the errors, misunderstandings and deficiencies which occurred in the creation of such a misleading term and definition. The book uses the findings and evidence from prior ME epidemics to support the case for caling the Lake Tahoe illness ME or ME type illness.
The invention of an insulting, useless and ineffective name such as 'Chronic Fatigue Syndrome' by Straus led to it being mocked, dismissed and ignored by medical doctors, scientific researchers, the NIH, the CDC and other similar bodies worldwide. It was deprived of proper research funding by governments, universities, foundations and philantropy bodies. There was no progress in scientific research and medical diagnostics for over 20 years. Sadly the medical and scientific findings from the Lake Tahoe epidemic were totally ignored and not replicated. The US government failed to follow up the viral, bacteria and mycotoxin, immune dysfunction, neurological, brain, and endocrine evidence from this Lake Tahoe epidemic and the Lyndonville epidemic (1985-1986) and other outbreaks in other states and countries in the 1990's and early 2000's. This failure by the US government and other governments continued up to the present day, and this created a lack of biomarker criteria for medical doctors and scientific researchers to work with. The scientific studies, recommended by the CDC in 1988 and in 1994 were not carried out or not properly funded by the US government. In 1990 research into ME revealed retrovirus sequences in patients suggesting retrovirus and possible HTLV infection - HTLV virus infection in ME (CFS) patients . This was ground breaking at the time, but it was not properly replicated by the CDC and NIH, and by other researchers and bodies. Dr. DeFreitas and the Wistar Institute offered to bring a CDC team of researchers to their lab to show them how they detected the retrovirus in ME patients. The CDC refused this offer. This neglect of important scientific findings was unexpected and quite surprising at the time. The CDC tried to suppress the retrovirus findings, dismissed and ridiculed the findings of Defreitas and others, tried to get DeFreitas fired from her job, and they discouraged and blocked other researchers from verifying her findings.
Dr. Michael Holmes in New Zealand found evidence of retrovirus infection in ME patients in the late 1980's and 1990's. He found reverse transcriptase, cells with convulted nuclei similar to AIDS, high levels of interferon and T cell abnormalities in ME patients - all suggesting retrovirus infection. His research work was suppressed and not funded after the CDC condemned DeFreitas in the USA. In 1994, Dr. Anthony Komaroff of Harvard Medical School reported that the brains of those people with ME were identical to those with AIDS dementia, when viewed with SPECT imaging. They were both completely different to normal healthy brains. He believed that ME cases were the result of viral infection of the brain and nervous system, similar to AIDS. (SPECT imaging of the brain: comparison of findings in patients with chronic fatigue syndrome, AIDS dementia complex, and major unipolar depression.
Schwartz R , Komaroff AL, Garada BM, Gleit M, Doolittle TH, Bates DW, Vasile RG, Holman BL. AJR Am J Roentgenol. 1994 Apr;162(4):943-51.). Dr. Seymour Grufferman and Dr. William Blattner found some evidence of HTLV infection in ME patients from the North Carolina Symphony in the early 1990's (Osler's Web, Hilary Johnson, pages 651-652). This was not followed up by the CDC and NIH.
In her book Plague, Dr. Judy Mikovitts managed to isolate a retrovirus in most ME patients, and she itemised the structure, operations and genetic material of this retrovirus. This retrovirus was a gamma retrovirus and was similar but different to the xmrv virus identified by Dr. Silverman. Researchers searched for Silverman's xmrv virus but failed to look for Mikovitt's gamma retrovirus. They found xmrv contamination. Researchers failed to use the exact methodologies used by Dr. Judy Mikovitts to isolate and study her gamma retrovirus, and thus they failed to find this gamma retrovirus in follow up studies, and this created some international controversey which has yet to be fully resolved. In 2013, Dr. Sidney Grossberg isolated a gamma retrovirus similar to Mikovitts's retrovirus, and he named it JHK virus. He has supplied details and methods for isolating this virus in ME patients and others. In October 2013, Dr. Hornig and Dr. Lipkin of Columbia University found retroviral sequences in ME patients, which corroborates the earlier findings of Mikovitts, De Freitas, Cheney, Peterson and Buchwald, surprised them and some other people. Yet 23 years ago, researchers found retrovirus sequences, and sadly these were never followed up and replicated properly. The implications of Defreitas', Holmes', Mikovitts', Cheney's Peterson's, Grossberg's, Lipkins' findings are very serious, there are undiagnosed retroviruses infecting the general population, and possible co-infections causing serious illness to many people. This is of great public concern. Dr. Judy Mikovitts and other scientists and doctors continue to push for further scientific research into retroviruses and the deployment of diagnostic kits and treatments. This failure to properly investigate retrovirus infections in ME patients, particularly severely ill patients, was a gross failure by government and has had serious repercussions for US citizens and millions of people worldwide.
During the late 1980's a new virus was discovered and called Human Herpes Virus 6a, and this infection was found in a significant percentages of CFS patients in studies at the time, and ever since. Yet the CDC, NIH and HHS failed to follow up these findings, replicate them across America and other countries, and establish causalities between immune dysfunctions and viral infections, and integrate them into the definition, diagnostics and biomarker data for CFS. The NIH and Department of Health also failed to encourage hospitals, clinics and labs to update their diagnostic equipment and methods to identify these new viruses. They also ignored growing evidence of toxic molds and mycotoxins in damp buildings and the fact that many people with CFS and respiratory illnesses had these infections. Thus the government failed on many counts to take basic measures to safeguard the health and well being of millions of Americans.
By 1994, the CDC published the Fukuda defintion and this created more confusion, as it lacked biomarkers, scientific evidence, replicated studies, clinical evidence and accurate diagnostics. This Fukuda criteria was so broad in its terms that it encompassed other similar illnesses. This in turn created different patient sets with different illnesses, all called CFS. This created heterogenous groups and conflicting research results, as one had different illnesses under one banner. After 1994, the US government was lobbied to clarify the situation and carry out intensive scientific research into CFS by several scientists, medical doctors and patient organisations, but the government neglected to do this on an adequate scale. By the mid to late 1990's, big insurance companies played a part in lobbying politicians and government health bodies to state CFS was a non illness and that it was psychiatric, in order to save money by not paying for patient diagnosis and treatments. This destroyed the lives of many patients and their families, leading to many thousands of deaths in the USA and other countries (which copied the USA). Straus's attempt to mock and belittle the illness with an insulting name had turned into a murder machine.
Deceit, Fraud and Criminality Certain individuals in the NIH and CDC played a part in blocking funding for ME (CFS) research during this period, as they both thought it was not worth researching. Dr. Bill Reeves of the CDC turned whistleblower in the late 1990's and said the following about fraud and misallocation of monies for CFS research:
“I believe that CDC has intentionally misrepresented monies allocated to CFS research and I cannot ethically support this,” wrote Dr. Reeves in his public statement. “The misrepresentations involve systematically charging between $400,000 and $2 million incurred by unrelated activities to CFS between 1995-97 and reporting to DHHS [Department of Health and Human Services], Congress and patients that the monies were used for CFS research.”
A 1999 report from the Inspector General of HHS found that of the $22.7 million the CDC charged to its CFS program between 1995 and 1998, less than half was spent on the illness. The report stated: “CDC spent significant portions of CFS funds on the costs of other programs and activities unrelated to CFS and failed to adequately document the relevance of other costs charged to the CFS program…As a result of these inappropriate charges, CDC officials provided inaccurate information to Congress regarding the use of CFS funds.” The Inspector General’s report found that $8.8 million was spent on non-CFS projects and that the documentation on an additional $4.1 million was so poor that it was impossible to determine whether they were used to support CFS research or not.
From fiscal 1995 through fiscal 1997, some $5.8 million that the CDC told Congress had been spent on CFS research actually went to other activities. Certain members in the CDC tried to cover this up at the time. There were no criminal prosecutions and court cases, and no one was fired or resigned, which was unusual when one considers the seriousness of the crimes and the fact that Americans were dying of the illness. Furthermore, Dr. Byron Hyde the famous Canadian doctor stated in his booklet ( A Brief History of Myalgic Encephalomyelitis ) that Dr. Straus (NIH) may have played some part in misdirecting or misappropriating the $34 million designated by the US government for ME (CFS) research in the late 1980s' and early 1990's. The $34 million was spent on researching other illnesses. Thats over $40 million in total which went missing from ME (CFS) research and was a huge loss to ME (CFS) research.
The CDC should be forced to refund this $40 million to ME and CFS research. Congressional hearings and federal court cases should be instigated to recover these monies and to prosecute certain people for criminal behaviour.
This failing by the US government, in particular the CDC and the NIH created a vacuum in medical science and scientific research, which had devastating consequences for millions of Americans and their families and communities. This is detailed in the book Osler's Web: Inside the Labyrinth of the Chronic Fatigue Syndrome Epidemic. Over time, some research, mostly private research funded by patients, ME organisations, some medical doctors, foundations and some Universities, found significant biological abnormalities and dysfunctions in the immune system, HPA axis, brain and nervous system, autonomic system, heart and circulation and the mitochondria and chronic infections in some cases. Yet these were not integrated into government policies and diagnostic and treatment criteria. The most fundamental question is this - Why was scientific and medical evidence of immune system dysfunctions and deficiencies, neurological and brain abnormalities, pathogen infections of the nervous system, muscles and intestines, mitochondria damage and dysfunctions, cardiac abnormalities, greater risks of specific Cancers, and HPA axis and endocrine abnormalities and dysfunctions ignored by the CDC, NIH, HHS and US government in the 1980's, 1990's and 2000's ?
The following Prime Time television programme was broadcast throughout the USA on the ABC channel in 1996. It outlined these facts to a national audience at the time.
The term 'Chronic Fatigue Syndrome' as defined by CDC is devoid of meaning, it is a useless, imprecise and ineffective term, it deliberately ommitted biomarkers and medical facts, and tells us nothing. It was invented by Dr. Straus (NIH) in 1988 to describe an ME type illness and recent ME type epidemic in Lake Tahoe. Yet it failed to describe the illness, define the illness or even name it properly.
Would one call Diabetes "Chronic Thirst Syndrome" or call Cancer "Chronic Weakness and Pain syndrome" or call Alzheimers disease "Chronic Forgetting Syndrome" or call Parkinsons disease "Chronic Tremor Syndrome" or call Anemia "Chronic Tiredness Syndrome" ?? The answer would be no as they are insulting, abusive and tell one nothing about the illness. Then why did Dr. Straus and some others use an insulting and abusive term such as "Chronic Fatigue Syndrome" to describe an ME type illness, an ME epdemic?
Dr. Straus' and Fukudas' CFS definition of 1994 was a disaster and lacked precision, accurate diagnostic critria and biomarkers and was so broad that it encompassed several other illnesses and created even more contradictions and confusion in the fields of medicine and scientific research. Calling ME all types of names whether it is 'Chronic Fatigue Syndrome', 'Chronic Weakness Syndrome', 'Chronic Headaches Syndrome' , 'Chronic Itch Syndrome', 'Chronic Coldness Syndrome', 'Chronic Pain Syndrome', etc. does not disguise the fact that it is ME or an ME type illness. This lack of precision, accuracy and specificity by the CDC, NIH and Dr. Straus meant that different illnesses were called CFS or ME, and this created heterogenous groups in research trials and medical practises, making it impossible to differentiate the genuine ME cases from the non ME cases. This confusion led to contradictory research findings, and to inconclusive markers for the illness. This in turn has led to contradiction and stagnation in scientific research and in medical / clinical practises, which exists to this day.
There is evidence that Dr. Straus acted maliciously to make the illness "evaporate" and disappear and become a non illness - click here to view letter exchanged between Dr. Straus and Dr. Fukuda shortly after the Fukuda definition was approved in 1994. He deliberately worked with others to omit the scientific and medical evidence, give the illness a bad name and a poor quality definition, belittle and denigrate it, deprive it of legitmacy and of research funding, and make the illness disappear. These actions contributed to the deaths of tens of thousands of patients. This was serious medical misconduct, possibly criminal.
Yet over time, the words CFS and ME were both used to describe the same illness, and it is customary to use one of the terms to describe the illness or a composite term such as ME . The term 'Chronic Fatigue and Immune Dysfunction Syndrome' or CFIDS is also used in the USA to describe the same illness. Using the term 'Chronic Fatigue' in the name of this illness is misleading, inaccurate and imprecise and has led to the illness being trivialised, mocked and belittled (even by some doctors). We have used the term ME on our web-site, though in some exceptional circumstances ME is used in order to cater for some patient organisations and past research papers.
If Dr. Stephen Straus (NIH) had decided to call the illness 'ME type illnesses' in 1988 and not CFS, and the NIH and CDC had properly researched the illness and funded global research into it, and other research institutions around the world copied them, the position would be much clearer for everyone today. We would have ME on the one hand and ME type illnesses which may have been named Neuro-Endocrine-Immune illness, Chronic HHV6a illness, Chronic Mold and Mycotoxin illness, Chronic Lyme disease with co-infections, Chronic Tick Borne illness, Chronic Mycoplasma disease, Chronic Immune Dysfunction Syndrome or Chronic HTLV illness all of which would be separate to ME. Though all would share many symptoms. This would facilitate precise and accurate diagnostics and treatments of patients and make the work of doctors, health bodies, insurance companies and goverments easier and more effective.
Dr. Straus did nothing to remedy his own errors and he played an important part in blocking government sponsored biological research into ME (CFS) for many years. He destroyed tens of thousands of lives. Dr. Byron Hyde the famous Canadian doctor stated in his booklet ( A Brief History of Myalgic Encephalomyelitis ) that Dr. Straus may have had some role in misdirecting or misappropriating the $34 million designated by the US government for ME (CFS) research in the late 1980s' and 1990's. The $34 million was spent on researching other illnesses. This was a huge loss to ME (CFS) research. The following video by Dr. Byron Hyde explains ME and the various medical and financial scandals.
Britain
In Britain, the name ME was used, not CFS. This was the case from 1956 to the early 1990's. British doctors and the British medical organisations, European and American doctors and medical orgnaisations accepted the findings of top ME doctors such as Dr. Donald Acheson, Dr, Melvin Ramsay, Dr. John Richardson, Dr. E. O'Sullivan, Dr. Galpin, Dr. Deisher, Dr. Parish, Dr. Shelokov, Dr. Henderson, Dr. Sigurdsson, Dr. Poskanzer, Dr. Gsell, Dr. Hill, Dr. Dowsett and Dr. Behan. These doctors had many years experience diagnosing, treating and researching ME. Some doctors even carried out autopsies on dead ME patients to determne the pathological aspects of the disease. These medical doctors and reseachers accumulated detailed medical facts and evidence over a few decades.There was a consensus within the medical community worldwide as to what ME was, and what it involved. Diagnostics and treatments and research efforts revolved around infections, immune dysfunctions, neurological dysfunctions, endocrine dysfunctions, and muclo-skeletal abnormalities and mitochondria dysfunctions.
In 1970 two psychiatrists McEvedy and Beard published a paper claiming that M.E. was a psychiatric disorder and that it was "all in the mind". The authors of this paper did not physically examine the patients, did not interview the patients, did not consult with the medical doctors and medical records of the patients. They merely superficially reviewed a few studies. The paper was a fraud, and was not based on a clinical examination of patients and biological and biomedical evidence and the biological testing and interview of patients. The paper was based on the presumptions and assumptions of two psychiatrists who knew nothing about the illness. The paper provoked a furious backlash from medical doctors and nurses who fell ill with M.E. Doctors, nurses and patients wrote letters in to the British prress and to medical and scientific journals rejecting the hypothesis of McEvedy and Beard. In 1978, The Royal Society of Medicine rejected the paper of McEvedy and Beard and their presumptions and stated that ME was a physical, biological illness involving infection and neurological, immune system and endocrine abnormalities - British Medical Journal, June 1978. This settled the matter in Britain and remained the position of the British Medical authorities and British government until the early 1990's. Dr. Byron Hyde a famous Canadian medical doctor wrote an interesting account of this in the following booklet - A Brief History of Myalgic Encephalomyelitis.
Then in 1991 and the early 1990's, a few psychiatrists managed to hijack the term ME (CFS) and falsely claimed it to be psychiatric illness and "all in the mind". The following nefarious activities were undertaken by a few psychiatrists in Britain:
These few psychiatrists cited the discredited and disgraced McEvedy paper from 1970 to support their theories and views in papers and alleged research.
The psychiatrists deliberately ignored and dismissed the medical and scientific findings of doctors such as Dr. Acheson, Dr. Ramsay, Dr. Richardson and many others from the 1950's to the 1980's, History of ME presented by Lisa Petrison to the CFSAC in 2014
The psychiatrists refused to test for biological evidence in their research. They based everything on their assumptions and presumptions.
The psychiatrists used their influence over government ministers, government departments, the press and media centres, the Medical Research Council, the Medical Council, the Royal Society of Medicine, the NHS, and government sponsored committees to convince them that ME (CFS) was psychiatric, "all in the mind", a non illness.
They used their influence over scientific and medical journals to block, censor and not publish scientific papers about the biological aspects of ME (CFS), encompassing immune system, neurological, endocrine, mitochondria abnormalities and infections in Britain, but were published in the USA, Canada, Australia, the EU and other countries. By the early 2000's they succeeded in getting some leading medical and scientific journals, outside Britain, to block and censor these research papers.
These psychiatrists used their influence over medical organisations in Britain and a few other countries to block all biological testing and all lab tests for ME patients. This deprived patients of essential lab tests, in order to determine the infections present and the biological dysfunctions and abnormalities present. This kept many patients in a limbo of sickness and deteriorating health for years and decades. This deprived ME patients of their basic Human Rights, Common law rights, and Constitutional rights. The NICE clinics in Britain are ineffective and a disgrace in their treatment of ME patients, as their ME diagnostics and criteria were developed by these psychiatrists and their supporters.
Scientific research into the biological causes and perpetuating factors in ME (CFS) was blocked by this small group of psychistrists "advising" and working within the Medical Research Council in Britain, over a period of twelve years. While psychiatric research into ME (CFS) was fully funded by the Medical Research Council.
They used their influence within the medical community in the USA and NIH and CDC to block research into biological causes, and to reduce the amount down to $5 milion per year, which is a tiny amount of research money compared to other similar illnesses, read http://me-ireland.com/research2.htm . This blocked new discoveries and new insights and the verification of biomarkers, and destroyed the lives of many ME patients.
The consequences of this psychiatrist inolvement were severe for ME patients and their families, as many ME (CFS) patients were often refused disability payments by insurance companies and by government. The patients were deprived of lab tests, and biological testing, and kept in a limbo of sickness and deteriorating health for years and decades. This led to loss of jobs, income, education, dignity, self-esteem, and to family break ups, suicides, and premature deaths from the health complications of ME (CFS), etc. for patients. It was a type of war against ME patients, and the source of great controversey in medicine. The psychiatrists became very wealthy from these activities and their work for insurance companies, drug companies and for government bodies. This is discussed and analysed in more detail in the Bogus Treatments section of this web site. Biological research into ME (CFS) continues to be blocked or severely under-funded in several countries in the present day. Patients and doctors have had to rely on private scientific research funded by patients, ME organisations, some medical doctors, foundations and some Universities. Recently, there has been a change in the policies of some governments who are now funding some biological research into the immune dysfunctions, pathogen infections, neurological abnormalities, HPA dysfunctions, mitochondria defects, etc. in ME, and ignoring the advice and influence of some psychiatrists. Research is under funded in Europe and North America, read http://me-ireland.com/research2.htm
Versions of ME and Versions of the false diagnosis CFS There are several versions of ME and CFS, including the CDC version, Oxford version, London version, NICE version, the Canadian Consensus version, the International Consensus (ICC) version, the Nightingale version, the Ramsay version, Dr. Peterson's and Dr. Cheney's version, and they all contradict each other. This is due to the false diagnosis of CFS which has no basis in medicine or science and is in the CDC version, Oxford version, NICE version and part of the Canadian version. The Ramsay version, Nightingale version, and ICC version and the ME version of Dr. Peterson and Dr. Cheney, the doctors who first diagnosed patients during the Lake Tahoe epidemic and witnessed the first outbreak of ME and wrongly called "CFS" are the most credible and complete versions. They are backed by science. Peterson and Cheney state that the illness they discovered has all of the primary determinants of ME plus the new evidence generated by Dr. Cheney and Dr. Peterson and the other scientific researchers and doctors who researched the Lake Tahoe epidemic from the mid 1980's to the mid 1990's. This evidence has been gathered and presented on the Lake Tahoe Epidemic (1984 - 85) page on this web site
The Nightingale version of ME supported by Dr. Hyde is also reliable and credible. It includes many of the findings of Peterson and Cheney and relies on the evidence of prior ME epidemics going back to the 1930's.
Their definitions of the illness were accurate and contained biomarkers, and have continued to be relevant in medical and scientific terms. These biomarkers and other biomarkers were found in subsequent research studies and patient cases. Unfortunately the CDC and NIH deliberately ignored the scientific findings and biomarkers of Cheney and Peterson for many years. Drs. Peterson and Cheney's findings and definitions and further follow up findings by other researchers were used in several successful ME clinics in the USA and abroad. They also played a key role in the development of the Canadian Consensus criteria 2003 and International Consensus criteria 2011, which are widely considered best international practises for diagnosing and treating the illness.
In summary, the Oxford version, London version, NICE version are all frauds invented by psychiatrists while the 1988 CDC version was the fraud created by Straus. They lacked scientific and medical evidence.
Chronic Fatigue in a larger context
The larger problem of 'Chronic Fatigue' from diagnosed and undiagnosed illnesses such as Diabetes, Cancer, MS, cardiac disease, adrenal disease, thyroid disease, Lyme disease, Vasculitis, parastical infections, AIDS, nutritional deficiencies (also in developed countries), heavy metal toxicity, organophosphate poisoning etc. which cause great fatigue and weakness remains a problem in many countries. Bierl et al. (1) found that 12% of the American population suffer from chronic fatigue which may be caused by one of these aforementioned illnesses or by a progression to a disabling illness, while 1.2% suffer from ME. The great problem is that many are undiagnosed and many people suffer unnecessarily. Doctor surveys consistently show that over 50% of patients complain of great fatigue while attending their doctor. The diagram below presents this problem of 'Chronic Fatigue' as it exists in many societies. ME is one of many physical, biomedical illnesses which involve 'chronic fatigue'. The term 'chronic fatigue' is far too general, and too easily open to misinterpretation and mis-diagnosis. It is important to differentiate which illness the patient actually suffers from.
"Severe intractable fatigue is endured by many people with a wide range of neuro-inflammatory, neuropsychiatric, and autoimmune disorders and cancer. Pathological fatigue is experienced by between 59 and 100 % of cancer sufferers depending on the clinical status of the disease [1]. Severe chronic fatigue is also experienced by many people with an autoimmune disease with 67 % of people with Sjögren’s disease [2], up to 76 % of patients with systemic lupus erythromatosis (SLE) [3] and upwards of 70 % of people with rheumatoid arthritis [4] suffering incapacitating levels of fatigue. Upwards of 80 % of multiple sclerosis patients suffer from incapacitating fatigue [5]. Beiske and Svensson reported that between 37 and 57 % of patients with Parkinson’s disease experience incapacitating fatigue [6]. Winward et al. reported data which strongly indicates that fatigue in stroke victims is a direct consequence of the cerebral infarct and not merely a consequence of increased effort during rehabilitation [7]. Severe fatigue was experienced by 87 % of people following major stroke 56 % of people following minor stroke and 29 % of people following a TIA [7]. Fatigue is commonplace in people following a myocardial infarction with almost 100 % of patients reporting debilitating levels of exhaustion. Interestingly, many patients reported severe fatigue without any concomitant signs of depression [8]. " Source: The Neuro-Immune Pathophysiology of Central and Peripheral Fatigue in Systemic Immune-Inflammatory and Neuro-Immune Diseases Morris et al. 2015.
There are common factors in all of these illnesses, involving activated immune pathways and inflammatory cytokines and inflammatory markers, and neuroinflammation, and high oxidative and nitrosative stress levels and damage, and mitochondria damage, damage to the nervous sytem, with or without infection(s)
Neurasthenia
The term ‘Neurashtenia’ was used in the late 19th century to describe an illness similar to ME. Neurasthenia has never been defined with precision and biomarkers, and it is a clinical non entity. It is well established as a means to not bother diagnosing a patient properly and not carry out appropriate laboratory and medical tests. And to neglect the patient. Neurasthenia is a term which was replaced regularly by doctors who took the time and effort to properly investigate, diagnose and test an illness.
This was the case when the name ‘Neuroasthenia’ was replaced during epidemics and clusters, notable replacements being ‘Epidemic Neuromyasthenia’, ‘Encephalitis’, ‘Akureyri Disease’, 'Iceland disease', ‘atypical poliomyelitis’, ‘poliomyelitis-like epidemic neuromyasthenia’, 'diencephalitis', ‘Abortive Poliomyelitis’, ‘Myalgic Encephalomyelitis’ from the 1920’s to the 1990’s. These were typical ME outbreaks. These various names describe a biological illness with underlying infections and biological dysfunctions and abnormalities. ‘Neurasthenia’ was falsely applied to these illnesses in the past, and encouraged by some medical authorities, but it’s ineffectiveness and failure as a term, a name, a definition, a description was and still is clear for all to see. Where the term ‘Neurasthenia’ was replaced during these epidemics, patients had a better chance of getting proper medical treatment. One should not describe physical, biological illnesses as psychiatric or psychological, but this basic rule of science and medicine has not fully been heeded in some quarters, even today. It is very clear that the use of the term ‘Neurasthenia’ is a means to dismiss patients, neglect patients, and give them a false and meaningless psychiatric diagnosis which totally ignores the underlying pathology, disease processes and biological dysfunctions.
Neurasthenia is a meaningless term, a clinical non entity, which should be removed from modern medical textbooks worldwide.
The Harmful Effects of CBT and GET in ME cases. The Inefficacy of CBT and GET.
There have been many research findings and clinical findings which show the harmful effects of CBT and GET and exertion in ME patients. In addition to this, the inefficacy of CBT and GET in terms of lack of full recovery, lack of return to normal function, lack of normal health (prior to illness), lack of return to sporting and other social activities, lack of return to full time employment or full time education or training has also been shown. This research is listed in the links below
Lorusso L, Mikhaylova SV, et al. Immunological aspects of chronic fatigue syndrome. Autoimmun Rev 2009; 8: 287-91.
Regional distribution of fatiguing illnesses in the United States: a pilot study. Cynthia Bierl, Rosane Nisenbaum, David C Hoaglin, Bonnie Randall, Ann-Britt Jones, Elizabeth R Unger and William C Reeves. Population Health Metrics 2004, 2:1
The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Lin JM, Resch SC, Brimmer DJ, Johnson A, Kennedy S, Burstein N, Simon CJ. Cost Eff Resour Alloc. 2011 Jan 21;9(1):1.
Structure of Causation and Continuation from a Scientific and Medical Perspective
(i) Can acute infections lead to chronic illness and infections, and other biological abnormalities ?
(ii) Chronic Infections & Chronic Immune system dysfunction with progression to Neuroinflammation and Neurological, Endocrine, Mitochondria, Vascular, Cardiac and GI dysfunctions and abnormalities
(i) Can acute infections lead to chronic illness and infections, and dyfunctional immune systems and other biological abnormalities ?
O'Connor et al. (2006) at the Centers for Disease Control and Prevention state . "Evidence now confirms that noncommunicable chronic diseases can stem from infectious agents. Furthermore, at least 13 of 39 recently described infectious agents induce chronic syndromes. Identifying the relationships can affect health across populations, creating opportunities to reduce the impact of chronic disease by preventing or treating infection.… infectious agents likely determine more cancers, immunemediated syndromes, neurodevelopmental disorders, and other chronic conditions than currently appreciated."
Science is continuing to uncover the impact of acute virus, mycoplasma and bacteria infections in the development of chronic illness. See Emerging infectious determinants of chronic diseases.
O'Connor SM, Taylor CE, Hughes JM. Emerg Infect Dis. 2006 Jul;12(7):1051-7.
"For example, fully 10% of people who suffered from E. coli food poisoning later developed a relatively infrequent life-threatening complication called hemolytic uremic syndrome (HUS) where their kidneys and other organs fail. (3) Approximately two-thirds of patients with Guillain-Barre syndrome, a suspected autoimmune syndrome, have a history of an antecedent respiratory tract or gastrointestinal infection. (4) Campylobacter infection is the most commonly identified precipitant of GBS and can be demonstrated in as many as 30 percent of cases. (5) Reactive arthritis (Reiter's syndrome) is another excellent example. Reactive arthritis is classically seen following infection with enteric pathogens such as Yersinia, Salmonella, Campylobacter and Shigella. (6) In a 2006 study, Alan S. Brown of Columbia University showed that prenatal infections such as rubella, influenza, and toxoplasmosis are all associated with higher incidence of schizophrenia. (7) Brown found a seven-fold increased risk of schizophrenia when mothers were exposed to influenza in the first trimester of gestation. One final example: a 2010 study concluded that cesarean delivery is associated with 1.8 times higher risk of celiac disease but not inflammatory bowel disease in children. (8)"
"A case-controlled study of residents of the Isle of Man found that 40 percent of people with sarcoidosis had been in contact with a person known to have the disease, compared with 1 to 2 percent of the control subjects.(12) Another study reported three cases of sarcoidosis among ten firefighters who apprenticed together.(13) A cluster of 13 cases of Parkinson's disease among a community of 592 people were reported in Israel, significantly more that would be expected by chance.(14) Research suggests that obesity is also an inflammatory disease caused by certain species of the Th1 pathogens. A study recently published in the New England Journal of Medicine found that a person's risk of becoming obese increases by 57% if they have a friend who becomes obese, and by 37% if their spouse becomes obese.(15) According to the researchers: "These clusters did not appear to be solely attributable to the selective formation of social ties among obese persons."
" Source:http://mpkb.org/home/pathogenesis/evidence_bacteria
Guillain-Barre syndrome
It is now well accepted by medical doctors and scientists worldwide (in 2016) that Guillain-Barre syndrome can be caused by viral infections or bacteria infections. This is confirmed by scientific research studies and clinical cases. This is an example of
(i) an acute disease causing a chronic disease, which is often misdiagnosed or not diagnosed
(ii)
a disease with different causative factors. It is caused by a number of different viruses or bacteria. This undermines the theory of one disease caused by only one germ.
In many cases the common cold is the cause, but other infections such as Zika virus, Epstein Barr and Herpes family infections which go into the nervous system and brain cause many cases of Guillain-Barre. These factors are being neglected by most doctors and healthcare systems and patients are often left to linger for years with no diagnosis or a misdiagnosis.
Jang et al. (2009) at St. Jude Children's Research Hospital, USA, discovered that an H5N1 Bird Flu (strain A/VN/1203/1204) infection in mice causes severe loss of tyrosine-hydroxylase positive dopaminergic neurons 60 days after infection by provoking a destructive autoimmune response, thus suggesting the infection by certain strains of flu might increase the risk of Parkinson's disease in humans. Source: Haeman, Jang; David Boltz; Katharine Sturm-Ramirez; Kennie R. Shepherd; Yun Jiao; Robert Webster; Richard J. Smeyne (2009-08-10). "Highly pathogenic H5N1 influenza virus can enter the central nervous system and induce neuroinflammation and neurodegeneration". Proceedings of the National Academy of Sciences 106 (33): 14063–8.
Research by Fonseca et al. (2015) found that infections can lead to chronic immune system dysfunctions which can persist for long periods afrer an infection is cleared. And these immune dysfunctions can make a person more vulnerable to other infections and inflammatory illnesses, such as allergies over time. Source: Fonseca DM, Hand TW, Han SJ, Gerner MY, Glatman Zaretsky A, Byrd AL, Harrison OJ, Ortiz AM, Quinones M, Trinchieri G, Brenchley JM, Brodsky IE, Germain RN, Randolph GJ, Belkaid Y. Microbiota-dependent sequelae of acute infection compromise tissue-specific immunityExternal Web Site Policy. Cell (2015).
Infection(s), chronically activated Immune system and Neuroinflammation & Oxidative and Nitrosative stress and damage in Neurological illnesses
Activated immune pathways and inflammatory cytokines and inflammatory markers, and neuroinflammation, and high oxidative and nitrosative stress levels and damage, and mitochondria damage, damage to the nervous system, with or without infection(s) has been found in neurodegenerative diseases such as Parkinsons, Alzheimers, MS and many others. This causes extreme fatigue and tiredness. This is also found in autoimmune diseases. And they are also found in ME and CFS, a neurological illness according to WHO, with immune system dysfunctions.
Morris G, Maes M. Oxidative and nitrosative stress and immune-inflammatory pathways in patients with Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Curr Neuropharmacol. 2014;12:168–85.
Morris G, Anderson G, Galecki P, Berk M, Maes M. A narrative review on the similarities and dissimilarities between myalgic encephalomyelitis/chronic fatigue syndrome (ME) and sickness behavior. BMC Med. 2013;11:64.
Morris G, Maes M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab Brain Dis 2014;29(1):19–36
The Complexity of Diagnosing Chronic Complex Illnesses involving Stealth Infections and Multiple Biological Dysfunctions
The following presentation was made to the Belgian Parliament in June 2014 by Dr. Richard Horowitz, an American medical doctor who has treated over 12,000 patients with Chronic Lyme, CFS, ME, Fibromyalgia and other infectious diseases https://www.youtube.com/watch?v=JSx3KdFaupA&t=8m40s
Chronic Infections and Reactivated latent viruses - A. Melvin Ramsay M.D
"Although the aetiological factor or factors have yet to be established, there are good grounds for postulating that persistent virus infection could be responsible. It is fully accepted that viruses such as herpes simplex and varicella-zoster remain in the tissues from the time of the initial invasion and can be isolated from nerve ganglia post-mortem; to these may be added measles virus, the persistence of which is responsible for subacute sclerosing panencephalitis that may appear several years after the attack and there is a considerable body of circumstantial evidence associating the virus with multiple sclerosis. There should surely be no difficulty in considering the possibility that other viruses may also persist in the tissues. In recent years routine antibody tests on patients suffering from myalgic encephalomyelitis have shown raised titres to Cocksackie B Group viruses. It is fully established that these viruses are the aetiological agents of 'Epidemic Myalgia' or 'Bornholm's Disease' and that, together with ECHO viruses, they comprise the commonest known virus invaders of the central nervous system. This must not be taken to imply that Cocksackie viruses are the sole agents of myalgic encephalo- myelitis since any generalised virus infection may be followed by a period of post-viral debility. Indeed, the particular invading microbial agent is probably not the most important factor. Recent work suggests that the key to the problem is likely to be found in the abnormal immunological response of the patient to the organism. " Source: MYALGIC ENCEPHALOMYELITIS : A Baffling Syndrome With a Tragic Aftermath. By A. Melvin Ramsay M.D., Hon Consultant Physician, Infectious Diseases Dept, Royal Free Hospital. [Published 1986]
The scientific research findings of Dr. Garth Nicolson show that co-infections are common in those people with chronic illness. We have provided listings of his research papers on this web site. In her speech at the International Congress of Autoimmunity, Amy Proal stated that of the Marshall Protocol subjects with Hashimoto's thyroiditis who participated in a survey, only 8% with Hashimoto's had Hashimoto's alone. The Hashimoto's patients had at least one, sometimes several comorbidities or co-infections. The same has been found in other patients with autoimmune and chronic illnesses, while they were receiving Marshal Protocol treatment.
The Marshall Protocol was devised by Professor Trevor Marshall. It is based on the premise that bacteria, fungi and viruses interact to cause chronic inflammatory illnesses. This includes MS, autoimmune illnesses, ME, neurological illnesses, Lyme disease, arthritis, rheumatism. Most of these illnesses involve disrupted and dysfunctional immune systems and chronic inflammatory conditions. Many of these infections are not picked up in standard tests, but they can inflict chronic inflammation and damage over time. A recent research paper at http://mpkb.org/home/publications/proal_autoimmunity_reviews_2009 explores this in more detail. The NIH has estimated that 90% of the cells in Homo sapiens are microbial and not human in origin. Some of these microbes create metabolites that interfere with the expression of genes associated with autoimmune disease.
Dr. Marshall has found that a dysfunctional VDR lies at the root of many cases of ME and CFS and other autoimmune and neurological illnesses. It leaves a person vulnerable to attack by viruses, bacteria and fungi and causes a deterioration in the patient over time. The following video lecture provides a good overview of the relationship between ME and chronic infections. https://www.youtube.com/watch?feature=player_embedded&v=2IMdAV6SIMU
(ii) Chronic Infections & Chronic Immune system dysfunction with progression to Neuroinflammation and Neurological, Endocrine, Mitochondria, Vascular, Cardiac and GI dysfunctions and abnormalities
One or more pathogens are suspected of being triggering agents for the illness. Cumulative pathogen load is important over time prior to ME onset and after ME onset. Immune system dysfunction is related to pathogen infection and pathogen load over time. Most of these viruses, mycoplasmas enteroviruses, chlamydia and other pathogens are not being detected in standard or outdated tests. Many doctors and research trials have failed to undertake intensive tests of spinal fluid and inflamed samples from dorsal root ganglia tissues, basal ganglia, brain stem, vagus nerve, spinal cord, cervical and lumbar nerve roots and peripheral nerves, and sites of brain lesions, intestinal tissues and muscle tissues to detect these pathogens. Many patients have been told they have no infection, when they actually have an infection which cannot be detected with outdated diagnostic equipment.
The immune system dysfunctions and abnormalities in ME patients makes them more susceptible to various infections. The acquired infection(s) will depend on one's geographical location and exposures, and one's genetic status and immune system status. Some of the following pathogens have been consistently found in ME patients:
Viruses include: Reactivated (latent) EBV virus, particularly in B cells, nervous system, glands and organs, HHV6a virus, Herpes family viruses 1-8, Parvovirus B-19, CMV, Coxsackie viruses, Enteroviruses, Ross river virus, Q fever virus, Stealth virus, JHK virus, Parainfluenza Virus-5 (PIV-5), Paramyxovirus and measles viruses of the Paramyxoviridae family, Cryptovirus, Borna virus, HTLV family viruses, HGRV virus in spinal fluids, nerve tissues, blood, brain, intestines, and muscles. Retroviruses are important, as Retrovirus sequences were found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in Columbia University in September 2013. Most of these viruses listed here would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Reactivated latent viruses include EBV, HERV-K18, Varicella-Zoster virus, Herpes family viruses 1-8, measles viruses of the Paramyxoviridae family. Some viral infections can reactivate latent viruses and undermine immune system functions. Mycoplasma: M. fermentans, M. penumoniae, M. hominis, M. penetrans, M. pirum, M. incognito. in intestines, spinal fluids, blood, brain, nerve tissues, muscles. These mycoplasmas would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Bacteria: Chronic Lyme disease, Ehrlichia, Bartonella, Brucella, Rickettsia, Chlamydia pneumonia, Staphylococcus spp. (live blood analysis), and Bacteria, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms in spinal fluids, intestines, blood, brain, nerve tissues, muscles. Intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism (Dr. Kenny De Meirleir). These bacteria would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Parasite: Cryptostrongylus pulmoni, Babesia, Candida, Giardia lamblia, Aspergillus Niger Molds, Bacteria and Mycotoxins in water damaged buildings: Stachybotrys family of molds, Cladosporium, Penicillium, Alternaria, Aspergillus, mycobacteria, Actinomycetes, Lipopolysaccharides (LPS), Microbial Volatile Organic Compounds (VOCs), Hemolysins.
These can cause chronic inflammatory immune response and immune dysfunction over time.
These infections may be causative, opportunistic or a co-factor in the illness.
A coroner's report of ME patient Sophia Mirza revealed that 4 out of 5 dorsal root ganglia were abnormal and showed disease. The coroner had not been able to find exactly what had caused this but the result was dorsal root ganglionitis – an inflammation. This suggests an infection of this area. An MRI scan or MRS scan or samples of this area would have revealed abnormalities, infections and inflammation while she was alive, but unfortunately this was never done. She was refused these tests by some doctors. These neurological abnormalities and extensive damage to the brain and nervous system were confirmed in another autopsy of a dead ME patient in 2017.
'Chronic fatigue syndrome (CFS) is characterized as a persistent, debilitating complex disorder of unknown etiology, whereby patients suffer from extreme fatigue, which often presents with symptoms that include chronic pain, depression, weakness, mood disturbances, and neuropsychological impairment. In this mini review and case report, we address central nervous system (CNS) involvement of CFS and present neuropathological autopsy findings from a patient who died with a prior diagnosis of CFS. Among the most remarkable pathological features of the case are focal areas of white matter loss, neurite beading, and neuritic pathology of axons in the white matter with axonal spheroids. Atypical neurons displaying aberrant sprouting processes in response to injury are observed throughout cortical gray and white matter. Abundant amyloid deposits identical to AD plaques with accompanying intracellular granular structures are observed as well. Neurofibrillary tangles are also present in the white matter of the frontal cortex, thalamus and basal ganglia. Taken together, these neuropathological findings warrant further studies into CNS disease associated with CFS.' CNS findings in chronic fatigue syndrome and a neuropathological case report. Kimberly Ferrero, Mitchell Silver, Alan Cocchetto, Eliezer Masliah, Dianne Langford
DOI: 10.1136/jim-2016-000390 Published 6 April 2017
There is a lot of evidence of viral and bacteria infections in ME , see Scientific Evidence and these may account for the damage to the brain and nervous system.
Recent ME subgroup recoveries from use of the medical drug Rituximab which is used for autoimmune illnesses and Cancers, strongly suggests autoimmunity involving B-cells and / or infection of B cells or B cell generation mechanisms as the key component in the illness, in addition to other immune system dysfunctions. Research shows close relationship between certain infections and the development of autoimmunity.
The current scientific research and clinical findings support the following conclusions:
Initiation of illness
In the diagram below, the virus or other pathogen may be
(a)exploiting an existing weakness in the immune system and/or genetic profile of the person brought about by several environmental and genetic factors
OR
(b)creating certain weaknesses in the immune system and / or genes, and these weaknesses persist over time and contribute to other immune system weaknesses and to opportunistic infections, and to further genetic effects, and a domino effect, affecting other body systems over time.
The end result is a chronic illness characterised by inflammation, infection, mitochondria defects and low energy, and neurological, cardiac, and HPA axis abnormalities, and continuing damage to cells, tissues and nerves, affecting many body parts, and causing deterioration of the patient over time.
- The Dubbo studies and other research findings mentioned above, and the scientific findings itemised in the Scientific Evidence section verify and corroborate this
- Kerr et al provide evidence of other triggers of (ME)CFS which include Parvovirus; C. pneumoniae; C. burnetti; toxin exposure and vaccination including MMR, pneumovax, influenza, hepatitis B, tetanus, typhoid and poliovirus (LD Devanur, JR Kerr. Journal of Clinical Virology 2006: 37(3):139-150).
And the findings of medical doctors, over many years, also corroborate this - see
Dr. Montoya's successful treatments
- Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. The part played by undiagnosed viruses and immune dysfunctions continues to be important in the illness.
- "The outbreak in Iceland was important, and provided some vital clues about the illness and the role of Enteroviruses.
"However,
children
in epidemic Neuromyasthenia areas
responded
to
poliomyelitis
vaccination
with
higher
antibody titres
than
in
other
areas
not
affected
by
the
poliomyelitis
epidemic,
as
if
these
children
had
already
been
exposed
to
an
agent
immunologically
similar
to
poliomyelitis
virus
(Sigurdsson,
Gudnad6ttir Petursson,
1958).
Thus,
the
agent
responsible
for
epidemic Neuromyasthenia would
appear
to
be
able
to
inhibit
the
pathological
effects
of
poliomyelitis
infection.
When
an
American
airman
was
affected
in
the
1955
epidemic
and
returned
home,
a
similar
secondary
epidemic
occurred
in
Pittsfield,
Massachusetts,
U.S.A.
(Hart,
1969:
Henderson
and
Shelokov,
1959)."
Many outbreaks of ME or epidemic Neuromyasthenia worldwide followed an outbreak of polio virus.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
- The
ME or epidemic Neuromyasthenia outbreak
at
Rockville,
U.S.A.
(Shelokov
et
al.,
1957),
was
associated
with
the
isolation,
from
a
number
of
the
patients,
of
Bethesda-Ballerup
paracolon
organisms
which
appear
to
have
triggered
off
the
disease
in
the
same
manners
as
infection
with
poliomyelitis
virus
pre-cipitated
other
epidemics.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
- Lake Tahoe outbreak
The Harvard-led research team found abnormal MRI brain scans, significant alterations in white blood cells counts and functioning, and signs of active infection with a recently discovered pathogen, HHV-6a. The illness was likely a “chronic, immunologically mediated inflammatory process of the central nervous system.”
Buchwald, D., Cheney, P., Peterson, D., Henry, B., Wormsley, S., Geiger, A., Ablashi, D., Komaroff, D.etc. 1992. A chronic illness characterized by fatigue, neurologic and immunologic disorders, and active Human Herpesvirus Type 6 Infection. Annals of Internal Medicine 1116: 103-13. (The seminal scientific research paper on the Lake Tahoe epidemic in the USA in the mid 1980's and the origin of the term CFS)
This is corroborated by the medical findings presented by Dr. Cheney, Dr. Peterson, Dr. Holmes, Dr. Komaroff, and others to the CDC and Federal health bodies and scientific journals during and after the Lake Tahoe outbreak which confirmed a rapidly spreading infectious disease with a short incubation period of one week or less which progressed to a chronic illness within 6 months. This incubation period narrows down the causative agent for the illness. High numbers of patients had HHV6a (then called HBLV), some had EBV, including reactivated EBV, some had CMV infection, some had serious Herpes simplex infections and some had measles infection. A significant number had several infections at the same time, including re-activated latent viruses.
All of these particular infections have an incubation period of greater than one week. The exception to this being latent versions of these viruses which can be reactivated within a day or a few days, and certainly less than one week. Some Enteroviruses have an incubation period of 1 week or less. Infection by bacteria, including brucella and other pathogens were also found in some patients, these typically have incubation periods of less than one week. Certain unusual immune system abnormalities and dysfunctions were found which undermined the body's ability to fight viruses and pathogens ; these may have been caused by the causative infectious agent.
The diagnosis of HHV6a was undermined by the fact that it was newly discovered and most doctors did not test for it and by outdated diagnostic technologies at the time which could not test for it. Click here on the following link to view some medical findings from the Lake Tahoe epidemic.
- Enteroviruses, indicated in most ME epidemics throughout history, were not tested for in the Lake Tahoe epidemic. Enteroviruses have been associated with ME since the 1930's. Names such as 'Epidemic Neuromyasthenia’, ‘Encephalitis’, ‘Akureyri Disease’, ‘atypical poliomyelitis’, 'Iceland disease', ‘poliomyelitis-like epidemic neuromyasthenia’, 'diencephalitis', 'diencephalitis', ‘Abortive Poliomyelitis’ were used to describe the illness prior to the term ‘Myalgic Encephalomyelitis’ being created by Dr. Melvin Ramsey in 1956. Enteroviruses were implicated in most epidemics from the 1930's to the present day.
" Primary M.E. is always an acute onset illness. Doctors A. Gilliam, A.
Melvin Ramsay and Elizabeth Dowsett (who assisted
in much of his later work,) John Richardson of
Newcastle-upon-Tyne, W.H. Lyle, Elizabeth Bell of
Ruckhill Hospital, James Mowbray of St Mary's, and
Peter Behan all believed that the majority of primary
M.E. patients fell ill following exposure to an enterovirus. (Poliovirus, ECHO, Coxsackie and the
numbered viruses are the significant viruses in this
group, but there are other enteroviruses that exist that
have been discovered in the past few decades that do
not appear in any textbook that I have perused.) I share
this belief that enteroviruses are a major cause. " Source:http://www.nightingale.ca/documents/Nightingale_ME_Definition_en.pdf
- Immune system abnormalities identified in Lake Tahoe epidemic - Low natural killer cell numbers and lowered cytotoxicity, B cell abnormalities, high levels of inflammatory cytokines, particularly IL-2. Drs. Komarroff, Cheney and Peterson believed a pathogen was involved in natural killer cell depletion, most likely a virus. These findings were never fully followed up by CDC and NIH and other research bodies in other countries since 1991
In the book Osler's Web: Inside the Labyrinth of the Chronic Fatigue Syndrome Epidemic by Hillary Johnson medical doctors in the USA found an unusually high number of B cell lymphomas in ME patients. Special scientific tests showed that these B-cell Lymphomas in ME patients were unusual types, not seen before. The researchers found B-cell deficiency in all patients, and a positive result on the kappa/lambda assay for a majority of these patients. After studying samples from approximately fifty patients, Wormsley estimated that the rate of clonal excess abnormality in the CFS patients from Nevada was at least 25 percent ('Oslers Web, by Hillary Johnson, Penguin Books 1997, page 94). This is significant as kappa/lambda light chains are the result of abnormalities within the bone marrow B-cell lineage. This has direct on B-cells and overall immunity, and susceptibility to Cancers. Recent scientific studies show that the incidence rate of non-Hodgkin's lymphoma is 0.02% in the United States, yet nearly 5% of CFS patients develop the disease. This is a significant risk factor.
-
During the Lake Tahoe outbreak, some patients had pre-existing chronic inflammatory immune response to mycotoxins and molds prior to developing full ME . Doctor's and researchers findings at the time confirmed most patients had severe allergies and some had sinusitis prior to the epidemic. These mycotoxins and molds play a part in instigating immune system dysfunctions and weaknesses, and scientific research now shows this to be the case. This may have caused patients to become more susceptible to viral and other infections during the Lake Tahoe epidemic. A weakened immune system always makes one more susceptible to infections, and this is paticularly true if this weakness exists over a long period of time. Interestingly some patients improved significantly and even recovered after they left the buildings containing molds and mycotoxins and got treatment for the viral and other infections. The link between chronic inflammatory immune response to mycotoxins and molds and increased susceptibility to viral infections and other infections is being researched by Dr. Shoemaker in the USA and by other scientific researchers.
- The virus may be incubating in and infecting the B-cells, thus initiating a viral infection, chronic immune system activation and dysfunctions, and autoimmunity simultaneously.
- The virus / pathogen may also be infecting the mitochondria or injuring it or blocking it and interrupting the krebs cycle and this is having a domino effect on the immune system and it's functions and signalling systems.
- The virus / pathogen may be chronically activating both inflammatory cytokines and microglia, creating a long-term inflammatory illness with significant pain and biological abnormalities.
- Blocks in the methylation cycle and in methylation can cause immune system abnormalities, including re-activation of latent viruses, thyroid and endocrine abnormalities, excess inflammation, antioxidant deficiencies, high homocysteine levels, arteriosclerosis and cardiac abnormalities, fatty liver, increased Cancer risk, neurotransmitter abnormalities and mood disorders, IBS, detoxification deficiency, multiple chemical sensitivity, cell growth and maintenance abnormalities. All of these are commonly found in most ME and CFS patients.
- Chronic mercury and nickel poisoning are consistently found in many ME patients. These heavy metals are destructive to the mitochondria, the immune system, the glands and HPA axis, the brain and the nervous system.
Progression to chronic state
- Progression to chronic illness 6 -12 months. Several body systems are adversely affected by this. There are immune system dysfunctions, increased oxidative and nitrosative stress, neuroinflammation, damaged mitochondria, and damage to the brain and nervous system, the glands and HPA axis, the heart, the blood vessels, the muscles, and the liver. All of these are inter-related body systems have feedback loops between them, contributing to a perpetuation of the illness, more dysfunctions and a worsening of the illness over time. Subgroups of patients depending on genetics, environment, geographical location, exposures to pathogens, vaccine reactions and toxins, length of time suffering illness and accumulation of biological dysfunctions and abnormalities, etc.
- The chronic state is usually arrived at through neglect of the patient, misdiagnosis, inadequte testing, psychiatric nonsense, out-dated diagnostic equipment, doctor's not knowing about ME , old, out-dated procedures, etc. and patients are left with chronic infections and several biological dysfunctions and abnormalities with an increased risk of premature death. This neglect and misdiagnosis imposes a huge burden on the patient and his / her family, and on the health system and on the government and taxpayers.
- Mitochondria Analysis & Cardiac Analysis
Source: Dr. Paul Cheney, The Cheney Clinic, USA.
Source: Dr. Paul Cheney, The Cheney Clinic, USA.
Source: Dr. Sarah Myhill. Myhill Medical Clinic, Wales.
Cardiomyopathy arising from mitochondria dysfunction, oxidative stress and infections
Source: Peckerman et al. 2003
- The virus / other pathogens and immune dysfunctions are reactivating latent endogenuous viruses with super antigens in some cases, which damage immune system function. The HERV viruses are implicated in this illness, as they are in other illnesses such as MS, AIDS, Rheumatoid arthritis. The herpes virus family 1-8 are also have latency states which become activated in some ME patients. Methylation cycle blocks and methylation failure can seriously undermine and weaken immune system function to the point that latent viruses can become active again.
- The virus / pathogen may be chronically activating both inflammatory cytokines and microglia and astrocytes, creating a long-term inflammatory illness with significant pain and biological abnormalities.
- Infection(s), chronically activated Immune system and Neuroinflammation & Oxidative and Nitrosative stress and damage in Neurological illnesses
Activated immune pathways and inflammatory cytokines and inflammatory markers, and neuroinflammation, and high oxidative and nitrosative stress levels and damage, and mitochondria damage, damage to the nervous system, with or without infection(s) has been found in neurodegenerative diseases such as Parkinsons, Alzheimers, MS and many others. This causes extreme fatigue and tiredness. This is also found in autoimmune diseases. And they are also found in ME and CFS, a neurological illness according to WHO, with immune system dysfunctions.
Morris G, Maes M. Oxidative and nitrosative stress and immune-inflammatory pathways in patients with Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Curr Neuropharmacol. 2014;12:168–85.
Morris G, Anderson G, Galecki P, Berk M, Maes M. A narrative review on the similarities and dissimilarities between myalgic encephalomyelitis/chronic fatigue syndrome (ME) and sickness behavior. BMC Med. 2013;11:64.
Morris G, Maes M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab Brain Dis 2014;29(1):19–36
For the patient, there is immune system dysfunction and autoimmunity, chronic infection(s), and central nervous system and ANS dysfunction and increased Cancer risk and increased heart attack risk as an outcome. Other pathogens can then ruthlessly exploit these weaknesses in the immune system and body, explaining the other infections and re-activation of latent viruses.
In her lecture in November 2009 at the University of Miami, Professor Nancy Klimas stated that most of the research in the USA and internationally found that the viruses found in ME all have several things in common: they infect the immune system and the neurological system; they are capable of causing latent infections and they can reactivate under certain conditions.
Click on the following links for diagrams depicting the chronic state of ME
Newly discovered Viruses involved in ME Scientific research points towards immune system damage caused by a virus or other pathogen or toxin which results in acquired immune weaknesses and dysfunctions, including chronic activation, which make patients more susceptible to viral infections and other infections. Research is consistently showing us chronic HHV-6a virus infection of the brain, brain stem, spine and nervous system and muscles and other body systems in 30% - 50% of ME patients - seeresearch into HHV-6a virus(in.pdf format). HHV-6a virus also attacks the immune system and can keep it in a permanently weakened state. The HHV-6a virus is ‘neurotropic’ meaning it prefers to live in brain tissue, spinal fluids and in nerve tissue, and is not detected in routine blood tests. There is no test for this in Ireland. This is very important as new research is showing nervous system dysfunction in most ME patients, and this is being confirmed by genetic studies. In particular, dysfunction and inflammation of the dorsal root ganglia and other peripheral ganglia in the nervous system and the brain stem is known to be a factor in ME. HHV-6a virus may be infecting these sites in the body in ME, thus leading to several domino effects and resultant abnormalities and dysfunctions. The books America's Biggest Cover-Up: 50 More Things Everyone Should Know About The Chronic Fatigue Syndrome Epidemic And Its Link To AIDS by Neenyah Ostrom and The Virus Within By Nicholas Regush explore the role of HHV-6a virus in ME in more depth. These two books provide fascinating reading.
Research now shows that HHV6avirus is also involved in AIDS and Multiple Sclerosis (MS). This finding is very serious and warrants further investigation and research. This is investigated in more depth in our Scientific Evidence section The above abnormalities help explain the severe exhaustion, muscle pains, exercise intolerance, physical weakness, loss of memory, mental confusion, infections, lymph swelling and other symptoms found in ME . It is widely believed that a breakdown in the immune system is the root cause of ME , and that infections may be causative, a co-factor or opportunistic in this illness. Recent research is slowly unravelling the root causes of ME - click here for the main research priorities.
Dr. John Chia in the USA has found enteroviral infections in a majority of ME patients. This confirms earlier findings from the 1950's, 1960's and 1970's concerning enteroviruses. These enteroviruses live in nerve tissues, the brain and nervous system, in muscles and in the intestines and cause significant damage and disability to a person over time. His scientific and clinical findings strongly suggest that many ME patients have entervirus infections and in some cases multiple viral infections (including HHV6a, CMV, Epstein Barr, enterovirus etc.), and that enteroviruses play a key role in the pathology of ME. You can view his findings by clicking here.
Retrovirus sequences have been found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in Autumn 2013, but this will require further analysis.
New scientific findings in the USA show that a significant percentage of ME patients are or were infected by Parainfluenza Virus-5 (PIV-5). This particular virus targets and degrades the STAT1 protein in the immune system, and this in turn leads to immune dysfunction. The destruction of STAT1 protein is one of the main features of ME, in addition to RnaseL abnormalities, PKR abnormalities, p53 protein abnormalities and Actin abnormalities. There is continuing scientific research to establish if this virus is causative, opportunistic or a co-factor in the illness. This research is being led by the National CFIDS Foundation in the USA which is continuing to fund and back excellent scientific research into ME. The Department of Homeland Security in the USA has also kindly assisted in this research and made some significant progress in terms of diagnosis and treatments. More information about these viruses can be found by clicking here.
Dr. Huber of Tufts University in the USA is carrying out research to determine if viral infections are leading to the reactivation of latent endogenous viruses such as HERV-K18 in ME patients. This is important as HERV-K18 has a super antigen which can cause the immune system to become over-activated and dysfunctional. Over time this can lead to a weakened immune system which is both activated and dysfunctional, and not capable of combatting other infections, and this is what we see in ME . This research will determine if this is what is occurring in ME and it is due to be published in 2013. Dr. De Meirleir and other researchers completed a ground breaking new study into HERV viruses and ME in Spring 2013. This strongly suggests HERV infection in the intestines and is detailed in the following paper Plasmacytoid Dendritic Cells in the Duodenum of Individuals Diagnosed with Myalgic Encephalomyelitis Are Uniquely Immunoreactive to Antibodies to Human Endogenous Retroviral Proteins. De Meirleir et al. in vivo27: 177-188 (2013). The re-activation of dormant endogenous viruses which are part of the human genome is a very recent and unexpected scientific finding and may explain the autoimmune aspects of ME and other illnesses. Research is ongoing into this.
Research from Australia shows that other less well known viruses such Ross river virus and Q fever virus may initiate ME. In addition, Epstein Barr virus was also examined in this study. (Peripheral blood gene expression in postinfective fatigue syndrome following from three different triggering infections.Galbraith S, Cameron B, Li H, Lau D, Vollmer-Conna U, Lloyd AR.. J Infect Dis. 2011 Nov 15;204(10):1632-40.). This supports the fact that several viruses are capable of causing ME and they can also act as a co-factor and /or opportunistic infection in the illness over time. They may also weaken immunity so as to reactivate latent viruses. This is the subject of ongoing scientific research in the context of pathogen / toxin subgroups.
Dr. John Martin of the Center for Complex Infectious Diseases has produced some research which suggests the involvement of stealth viruses in ME. You can read more about this at http://www.ccid.org/about.htm. It is a well accepted fact that there are many viruses and other pathogens not yet discovered by the medical and scientific community. The activation of the 2-5a synthetase / RnaseL anti-viral pathway in most ME patients suggests the involvement of viruses - discovered, partially discovered or recognised and undiscovered viruses. This is the subject of continuing scientific investigation and validation. It is important to re-state that viruses may be causative, opportunistic or a co-factor in this illness.
On the subect of chronic, hard to treat infections, and opportunistic infections, new research in 2014 has revealed that bacteria and other pathogens
have evolved to use a protein called 'Protein M' to block all antibodies produced by the human immune system. This makes humans more vulnerable to acute and chronic infections and can provide wrong antibody readings in tests. This remarkable discovery by scientists at the Scripps Research Institute in 2014 sheds new light on chronic bacteria infections in humans. As many ME patients have chronic infections, this information is important. Research is ongoing to uncover the part played by Protein M in chronic infections and chronic illnesses. Other protein markers used by pathogens are also being investigated.
See information on this at http://www.scripps.edu/news/press/2014/20140206lerner.html
Rituximab, B-cell abnormalities & Viral induced Autoimmunity & Cancers
The scientific findings show that B-cell abnormalities play a significant role in autoimmunity in ME, and the success of the drug Rituximab confirms these findings. The scientific research of Fluge and Mella in Norway show that depleting B-cells through Rituximab brings about recoveries in two thirds of patients. Yet this takes several months to achieve. Once Rituximab is withdrawn, the patients become ill again after a few months, as B-cell numbers increase. Viruses / mycoplasmas may be hiding in B-cells so as to infect patients and/or increasing B-cell production for infection purposes, indirectly causing both an autoimmune response and an ongoing infection. Dr. Martin Lerner (Michigan, USA) believes that anti-virals kill the viruses, but do not hit the B-cells which incubate the virus(es) and that Rituximab hits the B-cells, but has little effect on the viruses. This would explain why Rituximab improves ME patients after a few months, but when Rituximab is stopped, the patients deteriorate, as (infected) B cell populations increase again. Dr. Michael Pender in his paper CD8+ T-Cell Deficiency, Epstein-Barr Virus Infection, Vitamin D Deficiency, and Steps to Autoimmunity: A Unifying Hypothesis. Pender MP. Autoimmune Dis. 2012;2012:189096. postulates that EBV virus is capable of living inside B cells and using the machinery of these cells to replicate itself, and cause continuing infection, autoimmunity and immune dysfunction which could last for years and decades. He also states that reduced cytotoxic T cell function plays a key role in this, allowing EBV infection of B cells and other cells to continue. This is explored further in the following papers Could the Epstein-Barr Virus – Autoimmunity Hypothesis Help Explain Chronic Fatigue Syndrome ? and EBV I: A Deficient Immune Response, Increased Levels of Epstein-Barr Virus Opens Up EBV Question in Chronic Fatigue Syndrome Again. An excellent scientific paper produced by scientific researchers in Germany in 2014 shows the importance of chronic EBV infection, including persistent reactivation of latent EBV combined with a defective immune system. This plays a major role in ME (Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome.
Loebel M, Strohschein K, Giannini C, Koelsch U, Bauer S, Doebis C, Thomas S, Unterwalder N, von Baehr V, Reinke P, Knops M, Hanitsch LG, Meisel C, Volk HD, Scheibenbogen. Scientific analysis and discussion on http://simmaronresearch.com/2014/03/1591/ )
Scientific research in 2012 and 2013, by Dr. Bansal et al. in Britain shows unusual B cell abnormalities in ME patients, which suggest autoimmune factors.
' patients had greater numbers of naive B cells as a percentage of lymphocytes: 6·3 versus 3·9% in HC (P = 0·034), greater numbers of naive B cells as a percentage of B cells: 65 versus 47% in controls (P = 0·003), greater numbers of transitional B cells: 1·8 versus 0·8% in controls (P = 0·025) and reduced numbers of plasmablasts: 0·5 versus 0·9% in controls (P = 0·013). While the cause of these changes is unclear, we speculate whether they may suggest a subtle tendency to autoimmunity.'
(Bansal et al., (2013), Altered functional B cell subset populations in patients with chronic fatigue syndrome compared to healthy controls. Clinical & Experimental Immunology, 172: 73–80.)
This ties in to important scientific findings in the book Osler's Web: Inside the Labyrinth of the Chronic Fatigue Syndrome Epidemic by Hillary Johnson where medical doctors in the USA found an unusually high number of B cell lymphomas in ME patients. Special scientific tests showed that these B-cell Lymphomas in ME patients were unusual types, not seen before. The researchers also found B-cell deficiency in all patients, and a positive result on the kappa/lambda assay for a majority of these patients. This is significant as kappa/lambda light chains are the result of abnormalities within the bone marrow B-cell lineage. This has direct on B-cells and overall immunity, and susceptibility to Cancers.
Recent scientific studies show that the incidence rate of non-Hodgkin's lymphoma is 0.02% in the United States, yet nearly 5% of ME patients develop the disease. This is a significant risk factor. Furthermore, the increase in NF-Kb levels consistently found in most ME patients shows both an increase in inflammation and an increase in general Cancer risk. The National Cancer Institute, USA, has recently confirmed that there is a higher risk of these types of Cancers in ME patients ( Chang, C. M., Warren, J. L. and Engels, E. A. (2012), Chronic fatigue syndrome and subsequent risk of cancer among elderly US adults. Cancer, 118: 5929–5936. doi: 10.1002/cncr.27612 ). Among non-Hodgkin lymphoma subtypes, ME was associated with diffuse large B cell lymphoma and marginal zone lymphoma and B cell NHL not otherwise specified. They concluded that infection and chronic immune system dysfunction may play a role. Certainly the defects in B cells and defects in Natural Killer cell functions and numbers in addition to certain viral infections, and high levels of oxidative and nitrosative stress leaves many ME patients vulnerable to Cancers. Interestingly, a relationship between EBV infection and B cell Lymphomas has recently been found by researchers, and as both are found in ME patients, this may shed more light on ME and it's risk for factor for Cancer. The research paper can be viewed here at :
Snow AL, Lambert SL, Natkunam Y, Esquivel CO, Krams SM, Martinez OM (2006), EBV can protect latently infected B cell lymphomas from death receptor-induced apoptosis , J Immunol, Sep 1;177(5):3283-93.
HHV-6a virus which has been consistently found in high pecentages of ME patients has been found to be
associated with Hodgkin's lymphoma, acute lymphocytic leukemia,
African Burkitts lymphoma, and sarcoidosis, as well as
AIDS and Chronic Fatigue Syndrome. Lusso, P. et al.;
"In Vitro Cellular Tropism of Human B-Lymphotropic Virus(Human
Herpesvirus-6)"; Journal of Experimental Medicine 167:1659, May
1988). HHV-6a also destroys the B-cells of the immune system. This has been found in research carried out by Dr. Robert Gallo of the NIH in the USA and research by virologist Berch Henry, Nevada. This research is cited in the book 'Oslers Web', by Hillary Johnson. Furthermore, HHV6a virus can infect the immune system cells and the nervous system and brain, all of which are affected in ME. These findings and other findings strongly suggest that HHV6a plays a key role in ME.
Chronic Lyme disease which has been found in many ME and CFS patients can aso cause B cell Lymphomas via long term TH2 cytokine dominance. This is a factor which is often overlooked in ME and CFS.
Recent research shows some similarities between Cancer and ME. Immunological abnormalities such as a dysregulated RNase L pathway, hyperactive NF-kappaB, increased oxidative stress and reduced NK cytotoxicity, among others, are present in both Cancer and ME, as found by Meeus et al. in 2009 (Immunological similarities between cancer and chronic fatigue syndrome: the common link to fatigue? Meeus et al. (2009) Anticancer Res. 2009 Nov;29(11):4717-26.). This intriguing finding corroborates other research findings from around the world confirming increased Cancer risk in ME patients.
Studies also show a thyroid cancer rate of 1 to 15 per 100,000 but in ME patients the rate is 6,000 per 100,000 (The International ME Conference, 2007, London. Dr. Byron Hyde). This is remarkable and represents a very significant risk of thyroid cancer in ME . This risk may relate to the thyroid and HPA axis dysfunctions consistently found in ME , and the Herpes virus infections (which can cause certain cancers) and continuing immune system dysfunction and autoimmunity, and oxidative damage to mitochondria, DNA, cells and tissues over time.
Furthermore, Dr. Heng of Wayne State University (USA) found serious chromosone breakage in 100% of ME patients using spectral karyotyping. 53% were identified as having chromosome translocations, often considered to be a recognized stepping stone of the cancer initiation process. Details provided on the NCF web site at http://www.ncf-net.org/PressReleases.htm#nfc. Following from this, there is a need to test for internal radionuclides and radioactive particles in patients. These would be sources of regular exposure to radiation, capable of causing serious chromosone damage. Some good research articles concerning radiactive particles in the
environment and food chain and the development of Cancers, immune system, endocrine and neurological illnesses can be found at http://www.ncf-net.org/radiation.htm . The following paper analyses immune system abnormalities in ME and Cancer - Meeus M, Mistiaen W, Lambrecht L, Nijs J (2009), "Immunological similarities between cancer and chronic fatigue syndrome: the common link to fatigue?", Anticancer Res, Nov;29(11):4717-26, PMID: 20032425,
Dr. Uckun et al , recently published a paper 'Clinical Activity of Folinic Acid in Patients with Chronic Fatigue Syndrome' In this article, the researchers found that 94% of the ME patients had a B-cell immunodeficiency with a marked depletion of their CD19+IgM+ mature B-lymphocyte population. The CD19+IgM+ cells ranged from a low of 0.5% to a high of 53%. These researchers concluded that there was "a high incidence of severe B-cell immunodeficiency" in ME patients. This correlates to clinical and scientific findings in the book Osler's Web mentioned above.
Following the same subject of B-cell abnormalities, there are many similarities between ME and Idiopathic CD4+ T lymphocytopenia. They are so similar that some people believe they are the same illness or that it is a subgroup of ME. Idiopathic CD4+ T lymphocytopenia has also been called non-HIV AIDS, which means it is an immune system deficiency and dysfunction without the HIV virus. B-cell abnormalities occur in Idiopathic CD4+ T lymphocytopenia, in a similar manner to the way they occur in ME. These B-cell abnormalities may be the initiating factors for autoimmunity and certain Cancers.
Virus infections tend to have multiple effects on the human body. There is a strong belief that a virus and / or mycoplasma causes the abnormality in the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway OR a virus and / or mycoplasma infects the Mitochondria and interrupts krebs cycle function and this domino effects on the immune system. New scientific findings in the USA show that a significant percentage of ME patients are or were infected by Parainfluenza Virus-5 (PIV-5). This particular virus targets and degrades the STAT1 protein in the immune system, and this in turn leads to immune dysfunction. The destruction of STAT1 protein is one of the main features of ME, in addition to RnaseL abnormalities, PKR abnormalities, p53 protein abnormalities and Actin abnormalities. There is continuing scientific research to establish if this virus is causative, opportunistic or a co-factor in the illness.
These scientific findings are supported by other research findings showing a number of autoimmune disorders resulting from Mitochondria damage / destruction in ME which have direct effects on immune system functions and other bodily functions - these are outlined in the paper 'Acute Phase Phospholipids Related to the Cardiolipin of Mitochondria in the Sera of Patients With Chronic Fatigue Syndrome (ME ), Chronic Ciguatera Fish Poisoning (CCFP), and Other Diseases Attributed to Chemicals, Gulf War, and Marine Toxins' Yoshitsugi Hokama et al. Journal of Clinical Laboratory Analysis 22:99–105 (2008). Autoimmunity is further corroborated by other research which shows the IgM isotype of ACA was present in 95% of ME patients tested. This is an unusually high percentage and is an important finding. It suggests autoimmunity as anticardiolipin antibodies have consistently been found in autoimmune diseases and some infectious diseases. This correlates to autoimmune and B-cell abnormalities found in ME and to the effectiveness of the autoimmune drug Rituximab in clinical investigations. Rituximab, a chimeric monoclonal CD20 antibody, has been shown to normalize high ACA serum titers of patients with autoimmune systemic lupus erythematosus, rheumatoid arthritis, autoimmune thrombocytopenia, and autoimmune hemolytic anemia. New research by Knox et al. suggests that the viruses consistently found in ME share molecular homologies for autoimmune disease markers of the thyroid, lupus, MS. These viruses may be invovled in molecular mimicry of some autoimmune markers (Knox, K., et al. Systemic Leukotropic Herpesvirus Infections and Autoantibodies in Patients with Myalgic Encephalomyelitis – Chronic Fatigue Syndrome. 7th International Conference on HHV-6 and 7. March 1, 2011. Reston, VA.). This may be the cause of the autoimmune disorders found in ME, and it may also explain the effectiveness of Rituximab an autoimmune drug. This is fascinating as ME patients have many of the neurological symptoms found in autoimmune illnesses of the thyroid, Lupus and MS and other autoimmune conditions.
The microbiome is important in ME and researchers have found significant gut dysbiosis in ME patients. This has important implications fo the immune system and autoimmunity as over 60% of immune cells are in the GI tract. Autoimmune research shows that the genes of microbes have been found to interact with human genes and it is believed that this may play a role in chronic disease ; this is the subject of ongoing research. The role of genes from the microbial metagenome, and the sum total of their interactions with human genes, cells and tissues over time in ME patients need to be fully investigated. In this context, infection, inflammatory immune damage, oxidative stress, and molecular mimicry need to be carefully investigated.
There is also scientific evidence of Antilamin antibodies in many ME patients, which suggests autoimmunity. Recent scientific research at Yale University shows that Epstein Barr virus (which has been found in many ME patients) can cause autoimmune reactions in patients, and re-activate latent endogneous viruses. B-cell abnormalities are involved in this autoimmunity and this leads the author to suggest that the drug Rituximab may have a beneficial role in combatting viruses and autoimmunity. He also recommends anti-viral therapy for some autoimmune conditons. (Autoimmune disease: A role for new anti-viral therapies? Dreyfus DH. Autoimmun Rev. 2011 Dec;11(2):88-97.). This is important considering the role of B cell abnormalities, autoimmunity and the drug Rituximab in ME.
Research is showing that deep tissue infections and bone and cartilage infections and nerve system infections are playing a role in some autoimmune illnesses. These infections are difficult to diagnose and find and many patients have been neglected. The immune system is attacking its own tissues, cells, cartilage, bone, nerves, etc. trying to get at viruses, bacteria, mycoplasma, pathogens, with resultant inflammation and serious damage over time. Chronic infections would lead to cell depletion, tissue depletion, cartilage, connective tissue and bone depletion, nerve tissue depletion, etc. at the point of chronic immune activation and inflammation. And the immune system is creating antibodies to human cells, tissue, glands, etc. in the process, thus giving the impression of autoimmunity. Consultants should be taking biopsies of acute AND chronically inflamed tissues, cartilage, and bone and testing them for various infections ?
All of this begs the following questions:
- are certain viruses and pathogens infecting B cells and using the machinery of these cells to create autoimmune conditions, continuing infection and immune dysfunction OR
- are pathogens infecting
tissues, joints, bones, ligaments and causing immune system cells to react against these human tissues OR
-
are pathogens which integrate and contain human tissue / cell markers causing an autoimmune reaction OR
-
are pathogens mimicking human tissue / cell markers OR
-
is human cell debris from oxidative stress and damage causing an autoimmune response OR
-
do pathogens contain proteins or molecules which block immune response OR -
do pathogens contain similar proteins to that in surrounding human tissue OR - are polymorphisms,
mutations, predispositions, epigenetics, and changes in human genes from environmental factors and toxins causing autoimmunity
Autoimmune factors found in ME patients may be arising from one or more of these dynamics, this area is the subject of ongoing research.
In MS, B cells with these markers CD19+ CD27+ CD38- CD138- CD19+ CD38+ CD138+ in the spinal fluid and blood stimulate cytokines and immune activation and accompanying damage to the nervous system. The dysregulation of B cells enables the survival of certain viruses such as EBV which has been linked to the central nervous system (CNS) infection in MS (Opsahl and Kennedy, 2007). In such cases the presence of EBV infected B cells promotes the persistence of EBV in the brain (Buljevac et al., 2005) and accompanying neurological degneration in MS. And in ME, B cells have also been found to be dysregulated and EBV (active and latent) plays a role in some subgroups.
New research in 2012 into MS and autoimmunity factors has implications for ME, and many other autoimmune and neurological illnesses. The research suggests that latent viral infections hiding within the immune cells or other body cells, can produce chemicals (containing some RNA) which can cause the immune system to become highly activated, causing inflammation and accompanying damage to human cells, tissues, nerves, myelin sheaths, etc.. This gives the impression of an autoimmune response as it appears to be human cells and tissue being attacked by the immune system. The latent virus is not picked up in many diagnostic tests as it is not fully active, and latent viruses are rarely treated, thus a condition is allowed to become chronic and degenerative over time.
There is a famous case of a British woman who was diagnosed with MS in a hospital and received treatments for MS. After some time, she decided to do a chronic Lyme disease test. She tested positive for Lyme disease and received treatments for this and recovered. She did not have MS, but the results of brain scans and neurological tests for MS were identical to those for chronic Lyme disease. This a remarkable new medical finding, and shows that infections of the brain and nervous system can appear like the symptoms of MS - http://www.dailymail.co.uk/health/article-2343062/Mother-diagnosed-MS-facing-life-wheelchair-cured--discovered-symptoms-TICK-BITE.html. ME shares many characteristics with MS and chronic Lyme disease and many forms of encephalitis and Meningitis and they are classified as neurological illnesses. Yet there is a reluctance by doctors, specialists and researchers to decipher the reasons for the lesions in the brain and nervous system in ME, and the underlying infectious agents (both active and latent) which play a role in neurological illnesses.
Viral and other pathogen infections both active and latent play a key role in ME. In some instances, latent viruses have become reactivated through immune system weaknesses, methylation failure and other viral infections. And new intriguing research shows that HHV6a virus has become chromosonally integrated into the genes of some patients. These outcomes are affecting T-cells and B-cells in ways which have yet to be fully deciphered by scientists.
The work of Dr. Garth Nicolson suggests that mycoplasmas and viruses may be able to integrate host cell material into their own structures, thus initiating autoimmune responses by the immune system. This would lead to the immune system attacking areas of the body recently infected by these mycoplasmas and viruses.
The following research paper outlines biological similarities between Multiple Sclerosis and ME. There are intriguing similarities.
The following diagram by Knox et al. (2011) shows some of the autoimmunity factors found in ME.
Source: Knox, K., et al. Systemic Leukotropic Herpesvirus Infections and Autoantibodies in Patients with Myalgic Encephalomyelitis – Chronic Fatigue Syndrome. 7th International Conference on HHV-6 and 7. March 1, 2011. Reston, VA..
Subgroups - Matrixes of Viral, Mycoplasma and Pathogen infections, Immune system dysfunctions and autoimmunity factors, Mitochondria and Krebs cycle dysfunctions, Endocrine and HPA axis dysfunctions, Methylation Cycle blocks, Nervous system and Autonomic system dysfunctions & other biological abnormalities
The scientific findings in the Scientific Evidence section of this web site provide a lot of scientific evidence of viral and bacteria infections in ME patients. And the recent medical findings of Dr. Martin Lerner (USA), Dr. John Chia, Dr. Kenny De Meirleir (Belgium) and findings in Australia (Peripheral blood gene expression in postinfective fatigue syndrome following from three different triggering infections. Galbraith S, Cameron B, Li H, Lau D, Vollmer-Conna U, Lloyd AR.. J Infect Dis. 2011 Nov 15;204(10):1632-40.) strongly support the fact that there are viral infections in patients and in some cases these co-exist with chronic Lyme disease, mycoplasma, babesia, chlamydia and parasite infections. It strongly suggests that a number of viruses are capable of causing ME and they can also act as a co-factor and /or opportunistic infection in the illness over time. And these infections are accompanied by immune system dysfunctions and autoimmunity which persists over a long period of time. The findings of Knox et al. (2011) show the importance of Herpes infections in ME.
Source: Knox, K., et al. Systemic Leukotropic Herpesvirus Infections and Autoantibodies in Patients with Myalgic Encephalomyelitis – Chronic Fatigue Syndrome. 7th International Conference on HHV-6 and 7. March 1, 2011. Reston, VA..
The scientific and medical findings of Dr. John Chia in California confirm that viral and bacteria infections play a role in ME, and in subsets of ME patients. Dr. Chia's scientific findings are listed below.
The following videos are brief lectures by top medical doctors on the role of infections and immune system abnormalities. And the medical diagnosis and treatments used in some of the more successful ME clinics. They provide an excellent introduction to the illness and its treatment.
Dr. John Chia, is medical doctor based in California, who is world renowned for his work, particuarly with Enteroviruses. He has been treating ME pateints and researching the illness since the late 1990's. He has found that Enteroviruses are present in some subgroups of ME patients and that treating these Enterovirus infections can lead to significant improvement and recovery.
Enteroviruses have been associated with ME since the 1930's. Names such as 'Epidemic Neuromyasthenia’, ‘Encephalitis’, ‘Akureyri Disease’, ‘atypical poliomyelitis’, 'Iceland disease', ‘poliomyelitis-like epidemic neuromyasthenia’, 'diencephalitis', ‘Abortive Poliomyelitis’ were used to describe the illness prior to the term ‘Myalgic Encephalomyelitis’ being created by Dr. Melvin Ramsey in 1956. Enteroviruses were implicated in most epidemics from the 1930's to the present day.
" Primary M.E. is always an acute onset illness. Doctors A. Gilliam, A.
Melvin Ramsay and Elizabeth Dowsett (who assisted
in much of his later work,) John Richardson of
Newcastle-upon-Tyne, W.H. Lyle, Elizabeth Bell of
Ruckhill Hospital, James Mowbray of St Mary's, and
Peter Behan all believed that the majority of primary
M.E. patients fell ill following exposure to an enterovirus. (Poliovirus, ECHO, Coxsackie and the
numbered viruses are the significant viruses in this
group, but there are other enteroviruses that exist that
have been discovered in the past few decades that do
not appear in any textbook that I have perused.) I share
this belief that enteroviruses are a major cause. "
Dr. John Richardson, was a brilliant British doctor who spent over 30 years diagnosing and treating ME patients in Britain. He advised and mentored Dr. Byron Hyde. Dr. Melvin Ramsey is world famous for his contributions to ME research. Dr. Byron Hyde also has a good international reputation. ECHO 7 appears to be infecting significant numbers of ill people, including those with ME, ALS, Alzheimers, and Gulf War Illness.
His research paper provides some important insights - Chronic fatigue syndrome is associated with chronic enterovirus infection of the stomach.
Chia JK, Chia AY.
J Clin Pathol. 2008 Jan;61(1):43-8. Epub 2007 Sep 1. See diagram below:
Dr. John Chia presents his research findings up to the year 2011 to the National Institutes of Health (NIH) in the USA below:
Dr. Chia's work and findings are similar to those of John Richardson, a medical doctor who was based in Newcastle in England who treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.
The outbreak in Iceland was important, and provided some vital clues about the illness and the role of Enteroviruses.
"However,
children
in epidemic Neuromyasthenia areas
responded
to
poliomyelitis
vaccination
with
higher
antibody titres
than
in
other
areas
not
affected
by
the
poliomyelitis
epidemic,
as
if
these
children
had
already
been
exposed
to
an
agent
immunologically
similar
to
poliomyelitis
virus
(Sigurdsson,
Gudnad6ttir Petursson,
1958).
Thus,
the
agent
responsible
for
epidemic Neuromyasthenia would
appear
to
be
able
to
inhibit
the
pathological
effects
of
poliomyelitis
infection.
When
an
American
airman
was
affected
in
the
1955
epidemic
and
returned
home,
a
similar
secondary
epidemic
occurred
in
Pittsfield,
Massachusetts,
U.S.A.
(Hart,
1969:
Henderson
and
Shelokov,
1959)."
Many outbreaks of ME or epidemic Neuromyasthenia worldwide followed an outbreak of polio virus.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
Dr. Chia also presents his medical experiences in the videos below:
Dr. Martin Lerner is a medical doctor with 40 years experience. Certified by the American Board of Internal Medicine and is an Infectious Disease Specialist. Residency, Internal Medicine, Harvard Medical Services. Boston City Hospital and Barnes Hospital, St. Louis, MO. Washington University School of Medicine, M.D. Two Years, National Institute of Allergy and Infectious Diseases, Epidemiology Unit.
Alumni Awardee, Washington University School of Medicine.
Three years research fellow in infectious diseases at the Thorndike Memorial Laboratory, Boston City Hospital and Harvard Medical School under the direction of *Dr. Maxwell Finland, (founder of subspecialty infectious diseases). Chief of the Division of Infectious Diseases and Professor of Internal Medicine at Wayne State University School of Medicine, 1963-1982. Established a clinical virology laboratory and trained 33 physicians in the subspecialty of infectious diseases, Wayne State University, 1963-1982.
Dr. Kenny De Meirleir is medical doctor based in Belgium and in Nevada in the USA. He runs a well known medical clinic in Belgium and also works for the Whittemore Peterson Institute in Nevada in the USA. He has been treating ME patients and researching the illness since 1990. He has seen thousands of ME patients over the years. The medical and scientific findings of Dr. Kenny De Meirleir over 20 years support the role of infections and immune system abnormalities in ME . Lecture series by Dr. Kenny De Meirleir videos 1 - 20, created in 2012 and 2013. Specifically for medical doctors and hospital consultants.
Dr. Lucinda Bateman. Dr. Bateman is a highly respected and well experienced medical doctor who has been treating ME patients since the late 1990's. She is a medical graduate of the prestigious Johns Hopkins University in Maryland. Dr. Bateman runs an ME clinic in Utah in the USA which is visited by patients from many states throughout the USA. Her expertise in ME has been ackowledged by the US Government authorities and national patient organistions in the USA, who have asked her to serve on their committees and expert bodies.
Dr. Garth Nicolson is a professional scientific researcher based in Florida, USA. He has been researching pathogen infections and immune dysfunctions since the late 1980's. He runs the Institute for Molecular Medicine, and has carried out extensive research on hundreds of ME patients over the years. The scientific and medical findings of Dr. Garth Nicolson (USA) has consistently found that high percentages of ME patients have mycoplasma infections. A significant percentage also have co-infections including HHV6a and various bacteria infections. This correlates to illness severity. Dr. Nicolson also found evidence of immune dysfunctions. This ties into the work of other scientists and doctors who have consistently found viral, mycoplasma and other pathogen infections, along with immune dysfunction in ME patients.
Dr. Ritchie Shoemaker is a medical doctor based in Maryland, USA. He is one of the top experts on mycotoxins in the world. He has been treating ME patients since the late 1990's, and he believes that myctoxins are a major factor in some ME subgroups and in other illnesses. Mycotoxins are accepted by the CDC and NIH in the USA as being hazardous to health. Lecture below on the effects of chronic mycotoxins and mold exposure on the immune system, endocrine system and nervous system.
Dr. Paul Cheney, Dr. Meirleir and Dr. Peterson (mentioned above) are now using tests for mycotoxins as part of their diagnostics protocol for ME .
These medical doctors are clear that one must identify the infections present and identify the subsets of patients and then treat these infections so as to bring about recoveries from ME. It is well known that Cognitive Behaviour Therapy (CBT) and Graded Exercise Therapy (GET) cannot treat these infections in ME and thus cannot treat ME. This is a scientific and medical fact.
Further corroborating scientific evidence of viral infections and bacteria infections in ME is provided by Harvard Medical School Professor Anthony Komaroff and Neurologist Tracey Cho in their recent paper ' Role of Infection and Neurologic Dysfunction in Chronic Fatigue Syndrome.' Anthony L. Komaroff, Tracey A. Cho. Semin Neurol 2011; 31(3): 325-337. In this paper they reviewed scientific, medical and clinical findings over many years, and found evidence of infection by pathogens and immune dysfunction and neurological dysregulation in ME . These scientific findings are backed up by ground-breaking research in 2010 and 2011 by Dr. Martin Lerner, a highly esteemed medical doctor and researcher in the USA who has been treating / researching ME since the mid 1990's. Dr. Martin Lerner has found that some of these viruses have special characteristics:
- abortive lytic replication (EBV, CMV, HHV-6a) producing host cell apoptosis as described by Dr. Martin Lerner. - IgM antibody to non-structural gene products (resulting from abortive lytic replication) as described by Dr. Martin Lerner
- coexisting infection by bacteria, mycoplasma, babesia, chalmydia, Lymes disease.
- this type of infection causes an increase in a protein called dUTPase, a biomarker
Treating and eliminating these infections (over many months) has resulted in recoveries from ME. The above markers are a very important scientific discovery and could be one of the main bio-markers for ME.
In severely ill ME patients, Dr. Kenny De Meirleir has found intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism. The toxin H2S produces a lot of oxidative stress and damages mitochondria, the intestines, the immune system, nervous system and muscle tissue. It is a major factor in some subgroups of ME and may be the causative factor.
A parasite Cryptostrongylus pulmoni has been found in over 60% of ME patients in research and clinical practise. This particular parasite attacks the immune system, and causes immune dysregulation. It also secretes peptides which can adversely affect brain function, the nervous system, blood flow, the hypothalmus and the HPA axis in humans. All of these play a key role in ME. This infection may be causative or a co-factor or an opportunistic infection arising from immune system weaknesses.
Subgroups
The scientific findings support the existence of subgroups in ME, and these subgroups correlate to different matrixes of viral and pathogen infections, immune system dysfunctions, autoimmunity, HPA axis abnormalities, neurological dysfunctions, toxin loads, mitochondria and krebs cycle abnormalities, methylation cycle blocks, etc. This has been confirmed by some recent genetic research :
Lessons from Cancer
Many illnesses such as Cancer have subgroups, which means there are slight variations in the illness between sets of patients. This may be due to inherited genetic factors, environmental exposures, interactions of genes with the environment and mutations, polymorphisms and gene expression changes, differing immune systems and reactions, different pathogen exposures, and triggering mechanisms for the illness.
The eminent Dr. Stephen Holgate in Britain, stated recently there are 15 subgroups in breast Cancer and he believes that there are many subgroups in ME and CFS. There would be general agreement with him on this by most ME and CFS doctors and scientists and patients. There are some heterogeneous features in a distinct illness such as ME and CFS. As diagnostic methods and technologies improve over time, including genetic technologies, there will be (i) greater precision attained in the diagnosis of illnesses (ii) some illnesses will have their subgroups identified, classified and defined with greater precision (iii) illnesses which were once thought to be just one illness will be found to be a number of undiagnosed illnesses, and they will be split into separate illnesses as a result ; each having their own distinct bio-markers, genetic markers and symptoms. This will bring greater clarity into medical and scientific understandings of chronic physical illnesses such as ME.
For ME and other physical illnesses, these subgroups may be due to :
- inherited genetic factors, including genetic weaknesses and susceptibilities
- environmental exposures, including toxins and levels of oxidative stress in the body. And the interactions of genes with the environment, including toxins, pagthogen genes, and oxidative stress factors. The changes to the genes and to gene expressions.
- different triggering mechanisms for the illness
- the initial strength and status of one's immune system and it's susceptibility to viral / toxin induced immune dysfunction
- different pathogen exposures over time. This would include chronic sub-clinical focal infections and other infections.
- excessive chronic stress over a prolonged period of time, with a near constant 'fight or flight' response, causing shut down or slowing down of some body functions in order to survive, which disrupts glucose, oxygen and nutrient uptake at cellular level, and this in turn has negative and destructive effects on mitochondria function and the krebs cycle, immune system function, and HPA axis function. Adrenal exhaustion playing a significant role.. Many scientific studies have found that excessive stress lies at the root of many Cancers, heart attacks, strokes, diabetes, and other physical illnesses.
- geographical location
- the matrix of infections present in the patient. Including viruses, mycoplasmas, bacteria, candida, parasites.
- the matrix of Mitochondria and Krebs cycle dysfunctions, Immune system dysfunctions and autoimmunity factors, Endocrine and HPA axis dysfunctions, Methylation Cycle blocks, Central nervous system and Autonomic nervous system dysfunctions & other biological abnormalities present in the patient
- the progression of the illness over time. The accumulated damage and domino effects. And what stage of the illness a patient is in. Is it stage 1, 2 or 3.
For example ME has subgroups with the following characteristics
Subgroup 1 - virus a, virus d, mycoplasmas, mitochondria and krebs cycle abnormalities, central nervous system damage and brain damage, genetic factors a, r, l, n, methylation cycle blocks, immune system dysfunctions a, c and f, autoimmunity factors a, HPA axis dysfunctions, low circulating blood volume, sleep abnormalities, moderate heavy metal burden in body, Orthostatic intolerance and POTS, gastro-intestinal problems, brain lesions, serious mobility impairment, chronic allergies and/or sinusitis, stage 3 of the illness, serious cognitive impairment Subgroup 2 - virus e, parasites, chronic Lyme disease, mitochondria and krebs cycle abnormalities, central nervous system damage and brain damage, genetic factors r, f, q, b, methylation cycle blocks, immune system dysfunctions a, b, c and e, autoimmunity factors a,b, HPA axis dysfunctions, low circulating blood volume, sleep abnormalities, high heavy metal burden in body, skin rashes, gastro-intestinal problems, chronic pain, stage 1 of the illness, chronic allergies and/or sinusitis, higher Cancer risk Subgroup 3 - virus a, mycoplasmas, chlamydia, mitochondria and krebs cycle abnormalities, genetic factors l, n, d, h, methylation cycle blocks, central nervous system damage and brain damage, immune system dysfunctions a, b and d, autoimmunity factors a, b,d, HPA axis dysfunctions, low circulating blood volume, sleep abnormalities, moderate heavy metal burden in body, brain lesions, serious cognitive impairment, chronic allergies and/or sinusitis, Orthostatic intolerance and POTS, stage 2 of the illness, serious mobility impairment, cardiac abnormalities and higher heart attack risk Subgroup 4 - virus d, mycoplasmas, babesia, toxins b,e, mitochondria and krebs cycle abnormalities, genetic factors, b, l, f, e, methylation cycle blocks, central nervous system damage and brain damage, immune system dysfunctions a and f, HPA axis dysfunctions, sleep abnormalities, autoimmunity factors a, b, c, intestinal dysbiosis, moderate heavy metal burden in body, low circulating blood volume, gastro-intestinal problems, chronic allergies and/or sinusitis, chronic pain, stage 2 of the illness, Orthostatic intolerance and POTS, cardiac abnormalities and higher heart attack risk Subgroup 5 - mycoplasmas, chronic Lyme disease, mitochondria and krebs cycle abnormalities, toxins a,c,e, genetic factors s, h, g, e, central nervous system damage and brain damage, methylation cycle blocks, immune system dysfunctions a, b, d and e, HPA axis dysfunctions, gastro-intestinal problems, low circulating blood volume, high heavy metal burden in body, sleep abnormalities, skin rashes, chronic allergies and/or sinusitis, autoimmunity factors a,d, brain lesions, stage 3 of the illness, serious cognitive impairment, higher Cancer risk
Factors in common: immune system dysfunction a, mitochondria and krebs cycle abnormalities, methylation cycle blocks, HPA axis dysfunctions, low circulating blood volume, sleep abnormalities, autoimmunity factor a, heavy metal burden in body, central nervous system damage and brain damage, chronic allergies and/or sinusitis,. Subgroups differ slightly in infections, toxin exposures and loads, immune system dysfunctions, Orthostatic Intolerance and POTS, chronic pain and the degree of pain, brain lesions, gastro-intestinal problems, onset of the illness and age at onset, the duration of the illness and the degree of accumulated damage, the stage of the illness, and in heart attack risk and Cancer risk.
Genetics: some similarities between subgroups but some differences between subgroups. This may appear contradictory but it is not. Genetic expressions reflecting slightly different disease processes and biological dysfunctions and abnormalities in patients. This arising from different triggering mechanisms for the illness, different genetic inheritances and genetic weaknesses and susceptibilities, environmental exposures and genetic mutations and polymorphisms, oxidative stress factors, the initial strength and status of one's immune system and it's susceptibility to viral / toxin induced immune dysfunction, geographical location, different pathogen exposures, and the progression of the illness over time.
Treatment Implications: This will involve several diagnostic tests to identify all infections and immune system dysfunctions and autoimmunity factors, mitochondria and krebs cycle abnormalities, methylation cycle blocks, HPA axis abnormalities, and other biological abnormalities and dysfunctions in an ME patient. And then treating the main or primary abnormalities and dysfunctions and infections first. And after this, moving on to treat other biological abnormalities and dysfunctions. Dr. De Meirleir (Belgium) has had great success with Ampligen combined with anti-viral and anti-pathogen treatments in his clinic in Belgium. Firstly, all of the infections were identified through several intensive diagnostic tests. Then Ampligen was combined with specific anti-viral and anti-pathogen treatments.Treatment is given for several months and up to a year. The results were impressive, and patients recovered from ME. Dr. De Meirlier has stated that an eight-year follow-up of patients found that 92% had not relapsed. This is highly significant. This strongly indicates that Ampligen by itself may not be enough, but combining it with anti-viral and anti-pathogen treatments may bring about better improvement and a high probability of full recovey. This was reported in the AAME Conference of 2001, click here to view paper. This mode of treating several infections and dysfunctions at once is supported by Dr. Martin Lerner, Dr. Edward J. Conley and other ME specialist doctors.
The reactivation of latent and endogeneous viruses may be caused by pathogen infection / toxin exposure which adversely affects immune system function, and weakens it significantly and/or failures in methylation and/or mitochondria and the krebs cycle.
Scientific Research Priorities
(i) Developing and Building upon Past Research Findings & Biomarkers
use of electronic scans, imaging scans and signatures, spectral and spectroscopic scans and signatures, EMF scans and signatures and genetic signatures technologies to efficiently and accurately scan blood samples, spinal fluid samples, nerve tissues, brain sites, spinal sites, nervous system sites, intestinal tissues, thyroid gland sites, liver sites, adrenal gland sites, blood vessel tissues, and immune cells for infections and infectious signatures of known, and new and emerging viruses, bacteria, parasites and mycoplasmas
new technologies for rapidly identifying abnormalities in immune system cells and subsets, immune cell molecular markers, cytokines and cytokine networks and inflammatory markers such as C Reactive protein, TNF, NFκB and COX2. Integration of real time biological tracking technologies with smart technologies to assess progress or regress in patients.
technology to rapidly identify genetic markers, gene expression markers, genetic mutations and polymorphisms and their role in the illness
technology to rapidly identify abnormal molecular markers, miRNA's in the illness
proteomic markers, spinal fluid and other neurological markers
Metagenome. Deeper testing and analysis of viruses, mycoplasma and Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms
Microbiome factors influencing the immune system and nervous system, the illness development and perpetuation.
use of brain imaging technologies such as SPECT, PET, MRS, MRI, fMRI to detect brain abnormalities
use of Metabolomics to identify abnormalities in metabolism and cellular functions.
new imaging technologies and techniques to measure biological processes, functions and structures inside the human body. And differentiate healthy cells and tissues and activities from infected and inflamed cells and tissues and activities. Detect neuro-inflammation in the brain, spinal cord and nervous system.
testing of inflamed nerve tissues, muscle tissues and intestinal tissues
analysis of sub-cellular factors with wide ranging effects on the body - Mitochondria abnormalities and Methylation cycle blockages.
urinary and other metabolites
live blood analysis and analysis of multiple blood subsets, live infections, coagulation markers, and molecular markers.
Listing of Research findings and papers worldwide which need to be replicated or deciphered in more depth
The Dubbo Studies which were published in leading medical journals verify much of the above, and point to genetic factors, environmental factors and a post-infectious dysfunctional immune system as being the key factors in ME .
(a)Can acute infections lead to chronic infections and illnesses, and reactivations of latent viruses and bacteria migrating to other body organs ? and other biological abnormalities ?
O'Connor et al. (2006) at the Centers for Disease Control and Prevention state, “At least 13 of 39 recently described infectious agents induce chronic syndromes.” Science is continuing to uncover the impact of acute virus, mycoplasma and bacteria infections in the development of chronic illness. See Emerging infectious determinants of chronic diseases.
O'Connor SM, Taylor CE, Hughes JM. Emerg Infect Dis. 2006 Jul;12(7):1051-7.
"For example, fully 10% of people who suffered from E. coli food poisoning later developed a relatively infrequent life-threatening complication called hemolytic uremic syndrome (HUS) where their kidneys and other organs fail. (3) Approximately two-thirds of patients with Guillain-Barre syndrome, a suspected autoimmune syndrome, have a history of an antecedent respiratory tract or gastrointestinal infection. (4) Campylobacter infection is the most commonly identified precipitant of GBS and can be demonstrated in as many as 30 percent of cases. (5) Reactive arthritis (Reiter's syndrome) is another excellent example. Reactive arthritis is classically seen following infection with enteric pathogens such as Yersinia, Salmonella, Campylobacter and Shigella. (6) In a 2006 study, Alan S. Brown of Columbia University showed that prenatal infections such as rubella, influenza, and toxoplasmosis are all associated with higher incidence of schizophrenia. (7) Brown found a seven-fold increased risk of schizophrenia when mothers were exposed to influenza in the first trimester of gestation. One final example: a 2010 study concluded that cesarean delivery is associated with 1.8 times higher risk of celiac disease but not inflammatory bowel disease in children. (8)"
"A case-controlled study of residents of the Isle of Man found that 40 percent of people with sarcoidosis had been in contact with a person known to have the disease, compared with 1 to 2 percent of the control subjects.(12) Another study reported three cases of sarcoidosis among ten firefighters who apprenticed together.(13) A cluster of 13 cases of Parkinson's disease among a community of 592 people were reported in Israel, significantly more that would be expected by chance.(14) Research suggests that obesity is also an inflammatory disease caused by certain species of the Th1 pathogens. A study recently published in the New England Journal of Medicine found that a person's risk of becoming obese increases by 57% if they have a friend who becomes obese, and by 37% if their spouse becomes obese.(15) According to the researchers: "These clusters did not appear to be solely attributable to the selective formation of social ties among obese persons."
" Source:http://mpkb.org/home/pathogenesis/evidence_bacteria
Jang et al. (2009) at St. Jude Children's Research Hospital, USA, discovered that an H5N1 Bird Flu (strain A/VN/1203/1204) infection in mice causes severe loss of tyrosine-hydroxylase positive dopaminergic neurons 60 days after infection by provoking a destructive autoimmune response, thus suggesting the infection by certain strains of flu might increase the risk of Parkinson's disease in humans. Source: Haeman, Jang; David Boltz; Katharine Sturm-Ramirez; Kennie R. Shepherd; Yun Jiao; Robert Webster; Richard J. Smeyne (2009-08-10). "Highly pathogenic H5N1 influenza virus can enter the central nervous system and induce neuroinflammation and neurodegeneration". Proceedings of the National Academy of Sciences 106 (33): 14063–8.
The scientific research findings of Dr. Garth Nicolson show that co-infections are common in those people with chronic illness. We have provided listings of his research papers on this web site. In her speech at the International Congress of Autoimmunity, Amy Proal stated that of the Marshall Protocol subjects with Hashimoto's thyroiditis who participated in a survey, only 8% with Hashimoto's had Hashimoto's alone. The Hashimoto's patients had at least one, sometimes several comorbidities or co-infections. The same has been found in other patients with autoimmune and chronic illnesses, while they were receiving Marshal Protocol treatment.
(iii) Immune Dysfunctions and Associated Infections
Replication studies to further develop a biological systems model needs to be undertaken to explain the abnormalities in Immune system subsets & associated genes
(a) B cell abnormalities, Infections and Autoimmunity
A biological systems model needs to be developed through scientific trials, experiments and studies to explain
why does Rituximab, an anti-Cancer drug and autoimmune drug, lead to full recoveries from ME ? what are the biological and molecular pathways involved ? and are there other safer drugs which can do this ? are B-cells incubating and carrying a virus (latent or active) or mycoplasma or bacteria or other pathogen in ME patients causing an infection, immune activation, immune dysfunction and autoimmunity ? are B cells cells carrying cellular / genetic material of these pathogens ? Dr. Martin Lerner believes that B cells may be carriers or transport mechanisms for pathogens.
the exact role of B-cells and the various B-cell abnormalities, including:
all B cell markers in ME
B cell autoantibodies in ME
B cell autoimmune markers and instigators in ME.
B cell markers coding for inflammation and autoimmunity
B cell memory and formation in ME
bone marrow B-cell lineage in ME
genetic changes to B cell numbers and functions in ME
chronic EBV infection and other Herpes infection or incubation in the liver, the spleen, the thyroid gland, the joints, adrenal glands and the nervous system. And the effects of reactivation of EBV and other Herpes infections and migration to other body parts. Effects on B cells and other immune system subsets.
map the direct effects of the following on B cells, including infection of B cells and B cell activations / responses:
Viruses include: HHV6a virus, Herpes family viruses 1-8, Parvovirus B-19, CMV, Coxsackie viruses, Enteroviruses, Ross river virus, Q fever virus, Stealth virus, JHK virus, Parainfluenza Virus-5 (PIV-5), Paramyxovirus and measles viruses of the Paramyxoviridae family, Cryptovirus, Borna virus, HTLV family viruses, HGRV virus in spinal fluids, nerve tissues, blood, brain, intestines, and muscles. Retroviruses are important, as Retrovirus sequences were found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in Columbia University in September 2013. Most of these viruses listed here would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Reactivated latent viruses include EBV, HERV-K18, Varicella-Zoster virus, Herpes family viruses 1-8, measles viruses of the Paramyxoviridae family. Some viral infections can reactivate latent viruses and undermine immune system functions. Mycoplasma: M. fermentans, M. penumoniae, M. hominis, M. penetrans, M. pirum, M. incognito. in intestines, spinal fluids, blood, brain, nerve tissues, muscles. These mycoplasmas would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Bacteria: Chronic Lyme disease, Ehrlichia, Bartonella, Brucella, Rickettsia, Chlamydia pneumonia, Staphylococcus spp. (live blood analysis), and Bacteria, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms in spinal fluids, intestines, blood, brain, nerve tissues, muscles. Intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism (Dr. Kenny De Meirleir). These bacteria would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Parasite: Cryptostrongylus pulmoni, Babesia, Candida, Giardia lamblia, Aspergillus Niger Molds, Bacteria and Mycotoxins in water damaged buildings: Stachybotrys family of molds, Cladosporium, Penicillium, Alternaria, Aspergillus, mycobacteria, Actinomycetes, Lipopolysaccharides (LPS), Microbial Volatile Organic Compounds (VOCs), Hemolysins.
These can cause chronic inflammatory immune response and immune dysfunction over time.
Why is there Elevated B-cells with CD20 marker ? what is causing it ?
Why are naïve B cells a high percentage of all B cells. Why are there lowered levels of IL 21,12, and 27, which are involved in the maturation of B cells.?
why is the following found in ME patients ? what is causing it ? and can it be blocked, prevented, or reversed ?
' patients had greater numbers of naive B cells as a percentage of lymphocytes: 6·3 versus 3·9% in HC (P = 0·034), greater numbers of naive B cells as a percentage of B cells: 65 versus 47% in controls (P = 0·003), greater numbers of transitional B cells: 1·8 versus 0·8% in controls (P = 0·025) and reduced numbers of plasmablasts: 0·5 versus 0·9% in controls (P = 0·013). While the cause of these changes is unclear, we speculate whether they may suggest a subtle tendency to autoimmunity.'
(Bansal et al., (2013), Altered functional B cell subset populations in patients with chronic fatigue syndrome compared to healthy controls. Clinical & Experimental Immunology, 172: 73–80.)
are mature or immature B-cells or bone marrow B-cells implicated ?
is the "programming" or immunological memory of new or naieve B cells defective ? and if so, then why ?
what are the relationships between B Cell abnormalities in ME and increased risk of non Hodgkins Lymphoma and it's subtypes - diffuse large B cell lymphoma and marginal zone lymphoma ? In the book Osler's Web: Inside the Labyrinth of the Chronic Fatigue Syndrome Epidemic by Hillary Johnson medical doctors in the USA found an unusually high number of B cell lymphomas in ME patients. Special scientific tests showed that these B-cell Lymphomas in ME patients were unusual types, not seen before. The researchers found B-cell deficiency in all patients, and a positive result on the kappa/lambda assay for a majority of these patients. After studying samples from approximately fifty patients, Wormsley estimated that the rate of clonal excess abnormality in the CFS patients from Nevada was at least 25 percent ('Oslers Web, by Hillary Johnson, Penguin Books 1997, page 94). This is significant as kappa/lambda light chains are the result of abnormalities within the bone marrow B-cell lineage. This has direct on B-cells and overall immunity, and susceptibility to Cancers. Recent scientific studies show that the incidence rate of non-Hodgkin's lymphoma is 0.02% in the United States, yet nearly 5% of CFS patients develop the disease. This is a significant risk factor.
can the specific antibody markers and autoimmunity markers on B cells be identified
in ME patients ? and what role do they play in the overall illness ?
what role do the B cell receptors TLR7 and TLR9 have in this autoimmunity
Range of Autoimmunity Factors
are certain viruses and pathogens infecting B cells and using the machinery of these cells to create autoimmune conditions, continuing infection and immune dysfunction OR
are pathogens, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms infecting
tissues, joints, bones, ligaments and causing immune system cells to react against these human tissues OR
are pathogens which integrate and contain human tissue / cell markers causing an autoimmune reaction OR
are pathogens mimicking human tissue / cell markers OR
is human cell debris from oxidative stress and damage causing an autoimmune response OR
do pathogens contain proteins or molecules which block immune response OR do pathogens contain similar proteins to that in surrounding human tissue OR are polymorphisms,
mutations, predispositions, epigenetics, and changes in human genes from environmental factors and toxins causing autoimmunity
Autoimmune factors found in ME patients may be arising from one or more of these dynamics, this area is the subject of ongoing research.
Novel new ways for addressing this problem through new or existing medical treatments. Can pathogens or their components and mechanisms be blocked (at pahtogen or host level) or inactivated or precisely targeted and destroyed and/or can vaccines be developed ?
(b) ME is classified as a neuroligical illness and it has also been found to have significant immune system dysfunctions associated with pathogen infections. These pathogen infections have been found in the nervous system, and other body system and there is significant immune related inflammation and neurological inflammation. Investigate Viral, Bacteria, Lyme and Mycoplasma and other Pathogen infections of the nervous system, brain, intestines, blood, muscles, thyroid, liver, joints, organs, heart and blood vessels and immune system cells. Develop new and better tests over time.
The various infections of organs and body systems need to be identified. Establish how the virus or other pathogen is (a) exploiting an existing weakness in the immune system or genetic makeup of the person brought about by several environmental and genetic factors OR (b) creating certain weaknesses in the immune system, and these weaknesses persist over time and contribute to other immune system weaknesses and to opportunistic infections. The end result being chronic inflammation, infection, and continuing damage to cells, tissues and nerves, affecting many body parts, and causing deterioration of the patient.
This new research and findings would enable the chronic, complex, systemic and heterogenous nature of the illness to be understood by scientists and doctors.
(c) A biological systems model needs to be developed through scientific trials, experiments and studies to
Why does Ampligen, an immune system modulating drug lead to improvements and recoveries in certain ME subgroups ? what are the biological and molecular pathways involved ?
identify all the abnormalities in the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway, and the causes of such whether by visues / mycoplasmas / other pathogens / bio-chemicals. Can this process be blocked or inactivated or reversed through medical drugs.
Some of these have been deciphered here at: http://www.me-ireland.com/diag/3.htm#rn
map the relatioships between the the 2-5a synthetase / RnaseL anti-viral pathway and PKR pathway, STAT1 and other immune system subsets, the reactivation of latent endogenous viruses such as HERV-K18, the mitochondria and krebs cycle, and the methylation cycle blockages and the following :
Viruses include: HHV6a virus, Herpes family viruses 1-8, Parvovirus B-19, CMV, Coxsackie viruses, Ross river virus, Q fever virus, Stealth virus, JHK virus, Anellovirus, Parainfluenza Virus-5 (PIV-5), Paramyxovirus and measles viruses of the Paramyxoviridae family, Cryptovirus, Borna virus, Enteroviruses in intestines, spinal fluids, nerve tissues, blood, brain, muscles. Retrovirus sequences found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in September 2013, but this will require further analysis. Most of these viruses listed here would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Reactivated latent viruses include EBV, HERV-K18, Varicella-Zoster virus, Herpes family viruses 1-8, measles viruses of the Paramyxoviridae family Mycoplasma: M. fermentans, M. penumoniae, M. hominis, M. penetrans, M. pirum, M. incognito. in intestines, spinal fluids, blood, brain, nerve tissues, muscles. These mycoplasmas would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Bacteria: Chronic Lyme disease, Ehrlichia, Bartonella, Brucella, Rickettsia, Chlamydia pneumonia, Staphylococcus spp. (live blood analysis), and Bacteria, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms in spinal fluids, intestines, blood, brain, nerve tissues, muscles. Intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism (Dr. Kenny De Meirleir). These bacteria would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Parasite: Cryptostrongylus pulmoni, Babesia, Candida, Giardia lamblia, Aspergillus Niger Molds, Bacteria and Mycotoxins in water damaged buildings: Stachybotrys family of molds, Cladosporium, Penicillium, Alternaria, Aspergillus, mycobacteria, Actinomycetes, Lipopolysaccharides (LPS), Microbial Volatile Organic Compounds (VOCs), Hemolysins.
These can cause chronic inflammatory immune response and immune dysfunction over time.
And novel new ways for addressing this problem through new or existing medical treatments. Can viral components and mechanisms be blocked (at viral or host level) or inactivated or precisely targeted and destroyed and/or can vaccines be developed ?
Fragment 1, an ankyrin binding repeat domain which is known to
interact with various transport proteins. It is is capable of NF-kappaB mimicry. This may be interrupting the ion channels in the body.
"these results show that upon pathological cleavage of RNase L, fragments containing the ankyrin domain are released, which could be capable of interacting with selected members of the human ABC superfamily, preventing their interaction with the normal cognate ankyrin protein and hence impairing their proper cellular function. This interaction constitutes a common physiological mechanism explaining numerous and currently unexplained symptoms experienced by patients with CFIDS, which are otherwise totally unrelated."
Source: Interactions Between Rnase L Ankyrin-Like Domain and ABC Transporters as a Possible Origin for Pain, Ion Transport, CNS and Immune Disorders of Chronic Fatigue Immune Dysfunction Syndrome. Englebienne et al. 2001.
Is there a genetic cause of the abnormalities in the RnaseL anti-viral pathway and PKR pathway in ME ?
The book Chronic Fatigue Syndrome: A Biological Approach By Patrick Englebienne and Dr. Kenny De Meirleir provides some vital insights into the biological mechanisms of the RnaseL anti-viral pathway and PKR pathway in ME
Some medical drugs and supplements mentioned in the following link should be investigated further - www.me-ireland.com/treat/3.htm
(e) The role of VDR blockage on the immune system and it's vulnerability to viral, bacteria and other pathogen infections. Further testing and analyisis of the Marshall Protocol, and it's data on the VDR and pathogen infections, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms. How VDR becomes blocked, the extent of blockage and the effects of such on Immunity. http://mpkb.org/home/diseases
(f) The role and effects of theMTHFR gene mutation found in some ME and CFS patients
The Human Genome Project found that this gene has been found to be mutated or abnormal in many people. Some ME and CFS patients have this genetic abnormality. This causes methylation cycle blockage, immune system abnormalities, including re-activation of latent viruses, thyroid and endocrine abnormalities, excess inflammation, antioxidant deficiencies, high homocysteine levels, arteriosclerosis and cardiac abnormalities, fatty liver, increased Cancer risk, neurotransmitter abnormalities and mood disorders, IBS, detoxification deficiency, multiple chemical sensitivity, cell growth and maintenance abnormalities. All of these are commonly found in most ME and CFS patients. Testing Labs
- DNA Methylation Pathway with Methylation Pathway Analysis
(g) A biological systems model needs to be developed through scientific trials, experiments and studies to
map the full range of immune system dysfunctions and immuno-deficiencies present ? and why are they present ? what are the subgroups ? what are the biological pathways involved ? what has caused or altered these pathways and what is maintaining this over time ? and how are these immune system dysfunctions related to each other and to nervous system dysfunctions ?
what is the part played by microglia in immune dysfunctions and autoimmunity ? what are the biological pathways involved ?
what role do endorphins have
in immune dysfunctions and autoimmunity ? what are the biological pathways involved ?
what is the exact role played by toxins, inherited genes and genetic changes, and the dynamic between toxins and genes in the initiation of immune system dysfunctions ?
(h) The role played by Protein M in the immune dysfunctions in ME
Bacteria and other pathogens
have evolved to use a protein called 'Protein M' to block all antibodies produced by the human immune system. This remarkable discovery by scientists at the Scripps Research Institute in 2014 sheds new light on chronic bacteria infections in humans. As many ME patients have chronic infections, this information is important. Tests are being developed for Protein M. See paper below http://www.scripps.edu/news/press/2014/20140206lerner.html
Is Protein ME involved in the chronic infections in ME ?
Can Protein M be blocked or stopped by new medical drugs or new medical technologies ?
are other proteins, bio-chemicals and molecules being used by bacteria, viruses and other pathogens to block the antibody response or block other immune system activities ? If so, can these
proteins, bio-chemicals and molecules be blocked or stopped ?
(i) The Lake Tahoe outbreak of the mid 1980's was a significant develpment in the history of ME , and has had a major impact on research, diagnostics and treatments worldwide. The medical findings presented by Dr. Cheney, Dr. Peterson and others to the CDC and Federal health bodies and scientific journals during and after the Lake Tahoe outbreak confirmed a rapidly spreading infectious disease with a short incubation period of one week or less. This narrows down the causative agent for the illness.
Some patients had HHV6a (then called HBLV), some had EBV, including reactivated EBV, some had CMV infection, and some had serious Herpes simplex infections. All of these particular infections have an incubation period of a few weeks, not one week. The exception to this being latent versions of these viruses which can be reactivated within a day or a few days, and certainly less than one week. Infection by bacteria, including brucella and other pathogens were also found in patients. Certain unusual immune system abnormalities and dysfunctions were found which undermined the body's ability to fight viruses and pathogens. These persisted over time. All this points to immune system damage and to acquired immune weaknesses and dysfunctions, which made patients more susceptible to viral infection and other opportunistic infections. The diagnosis of HHV6a was undermined by the fact that it was newly discovered and most doctors did not test for it and by outdated diagnostic technologies at the time which could not test for it. Enteroviruses, indicated in most ME epidemics throughout history, were not tested for in the Lake Tahoe epidemic. The medical and scientific findings of the Lake Tahoe epidemic need to analysed further by researchers to determine research priorities and directions.
(j) the scientific and medical findings of Dr. Garth Nicolson (USA) has consistently found that high percentages of ME patients have mycoplasma infections. A significant percentage also have co-infections including HHV6a and various bacteria infections. This correlates to illness severity. Dr. Nicolson also found evidence of immune dysfunctions. This ties into the work of other scientists and doctors who have consistently found viral, mycoplasma and other pathogen infections, along with immune dysfunction in ME patients.
What is the exact relationship between mycoplasma / viral / pathogen infections, both active and latent, and immune system dysfunction, including progression to chronic (long-term) inflammation ?
Research is showing that deep tissue infections and bone and cartilage infections and nerve system infections are playing a key role in some autoimmune illnesses, including some forms of arthritis. These infections are difficult to diagnose and find and many patients have been neglected. The immune system is attacking its own tissues, cells, cartilage, bone, nerves, etc. trying to get at viruses, bacteria, mycoplasma, pathogens, with resultant inflammation and serious damage over time.Inflamed tissue / cartilage suggests an immune response to something, that something is usually a pathogen though it could be a toxin or allergen in some cases. Also, mycoplasmas and viruses may be able to integrate host cell material into their own structures, thus initiating autoimmune responses by the immune system.
This will require deeper analysis of inflamed tissues, and the composition of mycoplasmas and viruses which are involved in an infection. Including identification of host cell material within mycoplasmas and viruses and reactions by immune system cells to this. The real challenge for medicine and science is to find the pathogen or toxin which initiates and perpetuates ME, and also causes a chronic inflammatory autoimmune and how it does this.
(k) reactivation of latent viruses in ME provide an added dimension to this complex illness. Are latent viruses hiding within immune system cells and other body cells producing chemicals which lead to chronic and excessive immune system activation, inflammation and damage to cells, tissues, nerves, myelin sheaths, cartilgage over time ? And can this be tracked and analysed in the nervous system, including the brain, CNS and ANS, the muscles, intestines and other body organs ? Does the recent research findings by Dr Ute-Christiane Meier in relation to MS and viruses have relevance to ME, considering the fact that both illnesses are classified as neurological, and involve immune system dysfunctions and infections ?
The following research paper outlines biological similarities between Multiple Sclerosis and ME. There are intriguing similarities. These areas need to be more fully researched.
(l) Dr. John Chia's findings in relation to enterovirus infection of the intestines, muscles and nervous system needs to be replicated in order to establish what role enterovirus infection plays. Why do many patients with ME recover after treatment for enterovirus infection ? researchers will need to track infection biomarkers, immune system biomarkers, mitochondria and krebs cycle biomarkers, HPA axis biomarkers, and other biomarkers to establish how and why recovery takes place.
(n) Which immune deficiencies and defects, mentioned below, play the major role in getting ME and in the chronic phase of the illness. See diagrams below.
In the first diagram below, the virus or other pathogen may be (a) exploiting an existing weakness in the immune system or genetic makeup of the person brought about by several environmental and genetic factors OR (b) creating certain weaknesses in the immune system, and these weaknesses persist over time and contribute to other immune system weaknesses and to opportunistic infections. The end result is chronic inflammation, infection, and continuing damage to cells, tissues and nerves, affecting many body parts, and causing deterioration of the patient.
(o) why are there low natural killer cells in ME patients ? why have the natural killer cells got abnormally low cytotoxicity ? why is the function of natural killer cells compromised ? are the natural killer cells being infected by viruses / mycoplasmas / pathogens ? is deficient ATP a factor ? how can these abnormalities be reversed or remedied ?
(p) Microbiome. Over 70% of immune system cells are located in the gastrointestinal tract. What are the gastrointestinal abnormalities and dysfunctions in ME patients and how do these problems cause the immune dysfunctions and inflammations typically found in ME patients ? what are the correlations between gut dysbiosis AND immune system functions AND inflammation, including neurological inflammation ? what immune subsets are involved ? what inflammation markers are involved ? what is the role of the vagus nerve in this ? How can these abnormalities be remedied / treated / reversed ?
(q) the role of genes from the microbial metagenome, and the sum total of their interactions with human cells and tissues over time in ME patients. Which microbes and which genes are involved ? and what are their individual and cumulative effects ? what are the effects on the immune system, the mitcohondria, cell functions, and body system functions in ME ?
(r) why is perforin low in ME patients ? how can this abnormality be reversed or remedied ?
(s) a biological systems model needs to be developed through scientific trials, experiments and studies to
map the mitochondria defects and krebs cycle and ATP defects in ME in the context of viral infections, mycoplasma and other infections, excessive immune system activation over time, oxidative stress, free radicals, and Nitric Oxide abnormalities, toxins, chemicals and heavy metals. Can these processes be blocked or inactivated or reversed through medical drugs and/or nutritional supplements ?
what is the exact role of the mitochondria in the immune system dysfunctions found in ME
(t) what is causing the reduced IgG subclass 1 and 3 found in ME and Fibromyalgia ? does it undermine the immune system so that it cannot control latent infections and fight active infections ? and does this lead to a reactivation of latent viruses ?
(u) why does Low dose Naltrexone work in many ME cases and in other autoimmune diseases ? what are the exact biological pathways involved ? and what is the part played by microglia in immune system dysfunction ?
(v) A biological systems model needs to be developed to establish the role of Cryptostrongylus pulmoni infection of the body and accompanying immune system dysfunction. And novel new ways for addressing this problem through new or existing medical treatments. Can parasite components and mechanisms be blocked (at viral or host level) or inactivated or precisely targeted and destroyed and/or can vaccines be developed ?
(w) Applications of Immuno therapy: This usually involves extracting and then re-training / re-programming / restructuring various subsets of live immune cells (NK cells, Lymphocytes, T-cells, B-cells, Macrophages, Cytokines) and then injecting them back into the body. Studies show it is effective in some Cancers and chronic illnesses.
Other therapies involve using bacteria / virus / antigens to stimulate immune response or destroy another pathogen / tumour. Some topical creams can powerfully stimulate immune system components and subsets of immune cells.
How can we improve the precision and acuracy of Immuno therapy in ME patients ?
(x) Some medical drugs and supplements mentioned in the following link should be investigated further - www.me-ireland.com/treat/3.htm