The Law and Legal Position of ME / CFS Patients
Under British case law, ME / CFS is now accepted as a physical illness involving immune system abnormalities, infection and neurological dysfunction and it is not a psychiatric illness. This is now accepted by the British courts and judiciary. The following paper outlines the court cases which have led to this conclusion by the British law courts - http://www.meactionuk.org.uk/ME_Judgments.htm
The case law itself and the verdict of the Master of the Rolls is binding and can be cited in court cases in Britain and Ireland. It can also be cited in courts in the European Union (as UK is part of it). And it can be cited as precedents / persuasive evidence in the courts in the USA and Canada, Australia and commonwealth countries.
Spanish courts have decided that Fibromyalgia and Chronic Fatigue Syndrome are grounds for permanent disability, see court ruling details at The courts confirmed that fibromyalgia is grounds for declaring permanent disability . "The disability must be understood as the loss of capacity for serious anatomical or functional reductions that reduce or nullify the work capacity, and without that would inhibit the rating the possibility of recovery of working capacity when it is present as uncertain or very long term." This can be cited as legal precedent in courts in other European countries.
In 2013, in the USA, there was an important court case, where the judge determined that the Hepatitis B vaccine caused Chronic Fatigue Syndrome (ME/CFS) in one case. This was a significant development in that it showed that an inactivated or weakened pathogen in combination with a defective immune system and immune response can in some cases lead to ME/CFS. This outlines the importance of immune system defects in the illness, which have been found in many scientific research papers. Federal Court judgment in 2013, USA Hepatitis B vaccine has been ruled to cause chronic fatigue syndrome
Another legal case involved a CFS patient in the USA bringing RICO charges and breach of contract charges against an insurance company, for refusing to pay him disability benefits. He won the case on appeal Unum Life Insurance No Guarantee of Benefits. RICO charges and fraud charges provide an excellent means for patients to enforce their rights in the courts.
The recent actions of governments in Norway, Canada, Australia, and Japan in their acceptance of Canadian Consensus Critera (2003) or similar Biological based criteria (Japan) show that these governments legally accept ME / CFS as a physical illness requiring physical and biological diagnosis and treatments. This establishes a legal basis for biological based ME / CFS diagnosis and treatment and for public perceptions about the illness, which can be applied in other developed countries.
The Significance to ME/CFS of the Landmark Change to the UK Law on Consent
In March 2015 there was a landmark change to the UK law on consent which has significant implications for patients with ME/CFS. For full details of this change in the law please see the Supreme Court Judgement and related articles (1-8) below. Consider the following scenario: an NHS fatigue clinic doctor prescribes CBT/GET to a patient, informing them that research (eg PACE trial, 9 ) shows that CBT/GET are moderately effective at curing ME/CFS with no serious side effects and CBT/GET are recommended by NICE.
The patient consents to CBT/GET, trusting that what he has been told by his consultant is accurate and complete. However CBT/GET makes the patient considerably worse and he takes legal action. Under the previous law on consent:
"a doctor would not be negligent if the information given to a patient about treatment and/or a procedure was compatible with that which would be given by a responsible body of medical opinion, provided always that standard was considered reasonable by a Court." (4)
Therefore in the above scenario the doctor could have argued that he had complied with the law as he had followed " a responsible body of opinion", i.e. the view held by the UK psychiatric establishment and the NICE guidelines. But with this landmark change in the law, hiding behind "a reasonable body of opinion" is no longer an option: " The doctor is under a duty to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments. The test of materiality is whether, in the circumstances of the particular case, a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it" (1, para 87) (emphasis added)
Therefore a doctor can no longer just inform his patients of the risks based on the views of some researchers, he must inform his patients of all material risks found in allresearch and of alternative treatments. And ignorance of the facts is no excuse.
It should be noted that the Montgomery case, which led to this change in the law, was won not because the new law on consent was applied retrospectively but because the consultant was in breach of the GMC professional guidelines on consent which were extant at the time of the birth: (5) "By allowing the Appeal, it has been recognised that the Supreme Court is reflecting what the General Medical Council (GMC) has been setting out in its guidance on consent to medical treatment for many years - to fully advise a patient of the options for treatment, the risks of each option and the benefits of the option, and it is then for the patient, not the doctor, to advise which option they wish to choose."(10)
All doctors, researchers and health professionals who have for years prescribed CBT/GET without fully informing patients of risks, alternative treatments etc have been in breach of these GMC guidelines on consent.
In the UK , CBT is mainly prescribed as in the discredited PACE trial : "to change the behavioural and cognitive factorsassumed to be responsible for perpetuation of the participant’s symptoms and disability", whilst GET is prescribed to correct the assumed deconditioning and exercise intolerance caused by these wrong cognitions. (11, 16) (emphasis added) . However, the scientific evidence clearly shows these assumptions are wrong: the disease is not perpetuated by patients' aberrant cognitions and behaviour, it is perpetuated by on-going physical disease processes and therefore the use of CBT/GET as treatments for ME/CFS is scientifically invalid and potentially harmful.
That ME/CFS is a serious organic disease has been highlighted in two major, independent reports on ME/CFS published earlier this year in the US:
1. The Institute of Medicine report: "Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness" commissioned by the HHS, NIH, CDC, AHRQ and the FDA. (12)
2. The National Institute of Health Pathways to Prevention report: "Advancing the Research on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome". (13)
Their conclusions were based on comprehensive reviews of over 9000 peer reviewed research papers and testimony from expert researchers and clinicians in the field. Both reports concluded unequivocally that ME/CFS is a serious physical disease, not psychological:
"The literature review found sufficient evidence that ME/CFS is a disease with a physiologic basis. It is not, as many clinicians believe, a psychological problem that should not be taken seriously. A primary message of the report is that:
ME/CFS is a serious, chronic, complex, multisystem disease that frequently and dramatically limits the activities of affected patients. In its most severe form, this disease can consume the lives of those whom it afflicts.
This message should reassure the millions of people with the condition that their concerns are, indeed, legitimate, while sounding a wake-up call to clinicians and research funders that ME/CFS deserves closer attention."(14)
"Other key findings...postexertional malaise, where exertion from activity (even seemingly mild activity, such as walking or active cognition) can trigger a “collapse” or “relapse” of malaise that lasts days or longer, far in excess of what would normally be expected. There may be a delay between the trigger and the collapse. Physiologic abnormalities after exertion are seen, which supports patient reports that forcing a person to “push” themselves can lead to profound exacerbation of symptoms." (14)
"These new criteria highlight the critical importance of postexertional malaise, which is so characteristic that the committee believes that the concept of exertion intolerance should be part of a new name." (14)
The recent MEA Illness Management Survey Report clearly illustrates not only the physical risks but also the mental and emotional risks of CBT/GET. Some might argue that the MEA Report is merely patients' subjective experiences of these treatments and therefore has limited validity, but the PACE trial and other studies on which the NICE guidelines are based, also used subjective experiences to measure outcome. A court of law would surely find that this report provides evidence of risks which any "reasonable person" (1, para87) would "attach significance to" (1, para87) and therefore patients should also be informed of this kind of evidence of risk. (15)
One patient in the survey stated:
“It was torture, and abuse. Nothing more. The idea that ME can be exercised better when in actual fact it caused me to be much worse is reckless as it put my health at serious risk. I was made bedbound by GET. I did GET because I trusted the hospital consultant, he made me believe that it would work. Therefore my informed consent to do the course was achieved through coercion – coercion that was based on misinformation, false statistics and unsupported claims directly made by X and X. This kind of claim is medical fraud, and on balance an abuse of patients’ rights. Had I known the truth about GET I never would have done it.” ( 15, Patient 676, p136)
If this patient, and others in the survey, had been fully informed as was required by GMC professional guidelines, and is now required by law, it ishighly likely they wouldn't have consented to CBT/GET and immeasurable harm and suffering would have been avoided. It should be noted that the new law on consent also applies to other medical professionals, for example occupational therapists, physiotherapists, nurses, psychologists etc, who may also provide CBT/GET. They too could face litigation if they fail to adhere to this law:
" Doctors, and other healthcare professionals, are now under a clear duty to take reasonable care to ensure that patients are aware of all material risks. This judgment aligns the law with the guidance on consent set out by the General Medical Council."(6)
Finally, patients can now use this new law to help to defend themselves from being sectioned, or from being coerced into CBT/GET, and from health insurance companies wrongly claiming ME/CFS is a behavioural disorder curable with CBT/GET. So for example, if a patient is being coerced into doing CBT/GET or threatened with being sectioned, he can now demand to be fully informed of the risks of CBT/GET as is required by law. CBT/GET would then be seen to be a potentially dangerous and scientifically invalid treatment while the doctor's view that ME is a behavioural disorder would be unsustainable. Furthermore, the patient's refusal to consent to CBT/GET would be seen as a logical and sane response.
In conclusion, this new law on consent means the status quo cannot continue. UK doctors must now fully inform their patients of all the material risks of CBT/GET or risk litigation. For the sake of both patients and doctors, the Royal Colleges, BMA, GMC, NICE and NHS health boards must act urgently to ensure their members/employees have the knowledge and training to be able to comply with these new legal requirements and CBT/GET should be withdrawn.
Source: Sheila Campbell, October 2015, Britain.
REFERENCES
References 3, 4 and 5 provide an overview of this change in the law and are a good starting place.
7. BMJ Observations Ethics Man - Update on the UK law on consent, BMJ 2015;350:h1481, Daniel K Sokol, 16 March 2015 http://dx.doi.org/10.1136/bmj.h1481
8. BMJ News - Doctors should not cherry pick what information to give patients, court rules. BMJ 2015; 350, Clare Dyer, 13 March 2015 http://www.bmj.com/content/350/bmj.h1414
13. National Institutes of Health Pathways to Prevention Workshop: "Advancing the Research on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome"Ann Intern Med.2015;162(12):860-865. http://annals.org/article.aspx?articleid=2322804
14. Redefining the Chronic Fatigue Syndrome, Professor Theodore G. Ganiats MD, Ann Intern Med.2015;162(9):653-654. http://dx.doi.org/10.7326/M15-0357
The Harmful Effects of CBT and GET in ME / CFS cases. The Inefficacy of CBT and GET.
There have been many research findings and clinical findings which show the harmful effects of CBT and GET and exertion in ME / CFS patients. In addition to this, the inefficacy of CBT and GET in terms of lack of full recovery, lack of return to normal function, lack of normal health (prior to illness), lack of return to sporting and other social activities, lack of return to full time employment or full time education or training has also been shown. This research is listed in the links below
"The doctor is under a duty to take reasonable care to ensure that the patient is aware of any material risksinvolved in any recommended treatment, and of any reasonable alternative or variant treatments. The test of materiality is whether, in the circumstances of the particular case, a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it."
Therefore a doctor can no longer just inform his patients of the risks based on the views of some researchers, he must inform his patients of all material risks found in all research and of alternative treatments. And ignorance of the facts is no excuse.
The PACE trial Failure and The Controversies surrounding it The PACE trial in Britain had many deficiencies, flaws and defects which have been exposed by scientists, researchers and doctors and this brings its findings into disrepute. Yet some doctors and medical bodies who are ignorant of it's flaws, defects and failed results promote it and promote CBT and GET which have been proven ineffective, useless and also quite dangerous to the health of patients. This raises important legal issues as patients have continued to deteriorate and worsen over time from these ineffective and unproven treatments. Let us examine the PACE trial more closely.
Firstly, they engaged in trial by design by altering the outcome measures at the end of the trial so as to give the impression that an unsuccessful intervention was a success when in fact the results were so bad that several years later, no recovery rates have been published. This is detailed below:
Changes to the original recovery markers towards the end of the trial.
Original Recovery Criteria
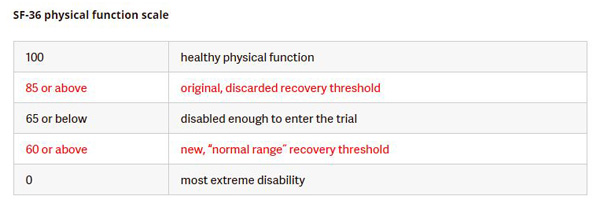
"Recovery" will be defined by meeting all four of the following criteria: (i) a Chalder Fatigue Questionnaire score of 3 or less [27], (ii) SF-36 physical Function score of 85 or above [47, 48], (iii) a CGI score of 1 [45], and (iv) the participant no longer meets Oxford criteria for CFS [2], CDC criteria for CFS [1] or the London criteria for ME [40]. Source:Original PACE Trial Recovery Protocols
(ii) SF-36 physical Function score of 85 or above
This was changed from 85 down to 60.
Their revision of the original outcome measures defining "recovery" makes it look like the researchers could not find any recovered patients using this criteria, so they changed this criteria towards the end of the trial so as to increase the likelihood of finding so called "recoveries". The new recovery marker 60 on the SF-36 scale was lower than the entry level marker to enter the trial 65 on the SF-36 scale , which means some patients, 13%, who entered the trial were already "recovered" according to this criteria before the PACE trial began. This also created the contradiction where a participant could worsen and deteriorate (drop from 65 to 60) and be deemed "recovered" at the end of the trial.
This makes a total nonsense out of their term "recovery", completely undermining the results of the PACE trial. It is considererd unethical, un-scientific and unusual to alter the set or agreed primary outcome criteria of a trial during the trial or at the end of a trial. In addition, this revision of the criteria defining "recovery" contradicts the criteria used in other studies into CBT and GET in ME trials (Bleijenberg et al. BMJ: 2005 January 1; 330: (7481):14). So a person could be very ill with ME and be disabled and they would claim him / her to be "recovered" in the PACE trial, which was a distortion of facts, a ridiculous lie. This alleged 'recovered' state is similar to the average for patients with Class II congestive heart failure.
It is important to be aware that the figure of 60 for "recovery" was used by the Investigators specifically for the
PACE trial and it contradicts how they themselves previously defined markers of recovery in the same disorder
using the same measure: in 2007 they stated: "A patient had to score 80 or higher to be considered as recovered"
(Psychother Psychosom 2007:76:171-176) and in 2009 their Dutch colleagues asserted: "A cut-off of less than or
equal to 65 was considered to reflect severe problems with physical functioning" (European Journal of Public
Health 2009:20:3:251-257).
(i) A Chalder Fatigue Questionnaire score of 3 or less
a Chalder Fatigue Questionnaire score of 3 or less out of maximum 11 to mean recovery was originaly set in the PACE protocol. Patients had to have scored 6 or higher on the 11-point fatigue scale to qualify for the trial and their fatigue could worsen during the trial up to a score of 9 — close to the maximum — and yet they would be classed as within the “normal range” for fatigue. This so called 'normal range' was alleged by he authors to mean recovery. So a person could be very ill with ME and be disabled and they would claim him / her to be "recovered" according to this criteria in the PACE trial, which was a distortion of facts, a ridiculous lie.
Original Recovery criteria: 3 or less (Bimodal scale). Later changed towards the end of the trial to 18 or less (Likert scale) Entry critera: 6 or higher to gain entry (Bimodal scale). Later changed towards the end of the trial to 12 or higher (Likert scale). Using new Likert scale a participant could be improved or recovered before the trial began
This scale was later changed towards the end of the trial from bimodal to Likert. They claimed 18 or less out of maximum of 33 denoted recovery towards the end of the trial - "We therefore considered a score of 18 (highest integral score below the mean plus 1s.D.) or less as within the normal range for fatigue." The figure for 18 or less was far higher than 6 or less which is its direct translation from the original protocol. Yet 12 was the (revised) entry criteria, and an increase to 18 meant worsening of the ilness, so a participant could worsen during the PACE trial and they would claim him / her to be "recovered" using the new criteria. This also created the contradiction where a participant t could be deemed "recovered" according to this criteria before the PACE trial began. A person could be very ill with ME and be disabled and they would claim him / her to be "recovered" in the PACE trial, which was a distortion of facts, a ridiculous lie. This alleged 'recovered' state is similar to the average for patients with Class II congestive heart failure. None achieved the original recovery protocol of 3 or less in the original protocol or 6 or less in the new amended protocol.
(iii) CGI score of 1
This a scale of 1 to 7, with 1 representing recovery and 7 severe illness and disability.
This was changed to 1 or 2 to mean recovery, with 2 representing the 'process of recovery' towards the end of the trial. This inclusion of 2 was not backed up by scientific studies and references. This change or relaxation of the criteria had the objective of finding more so called "recoveries".
(iv) The participant no longer meets Oxford criteria for CFS, CDC criteria for CFS or the London criteria for ME.
' The last protocol requirement for "recovery"—not meeting any of the three case definitions used in the study–was now divided into less and more restrictive sub-categories. Presuming participants met the relaxed fatigue, physical function, and Clinical Global Impression thresholds, those who no longer met the Oxford criteria were now defined as having achieved "trial recovery," even if they still met one of the other two case definitions, the CDC's chronic fatigue syndrome case definition and the ME definition. Those who fulfilled the protocol's stricter criteria of not meeting any of the three case definitions were now defined as having achieved "clinical recovery." The authors did not explain when or why they decided to divide this category into two.
After these multiple relaxations of the protocol definition of “recovery,” the paper reported the full data for the less restrictive category of “trial recovery,” not the more restrictive category of “clinical recovery.” The authors found that the odds of “trial recovery” in the cognitive behavior therapy and graded exercise therapy arms were more than triple those in the adaptive pacing therapy and specialist medical care arms. They did not report having conducted any sensitivity analyses to measure the impact of all the changes in protocol definition of “recovery' '
Source: David Tuller, TRIAL BY ERROR: The Troubling Case of the PACE Chronic Fatigue Syndrome Study
The PACE authors abandoned all of the four criteria specified in the study protocol and replaced them with far weaker ones towards the end of the trial. And they did no sensitivity analysis of the effect of these changes. They provided no detailed explanations and citations to back up these changes. They did not publish the findings from the original protocol and the changed protocol, so that comparisons could be made. This is unscientific and undermines its credibility and validity.
New "recovery" criteria towards the end of the trial
Changing the criteria for recovery or "normal range" from the orignal protocol which used well established and widely used figures (80 - 85 or more on the SF-36 and 3 or less on the Chalder scale) to a new protocol using the mean (average) figure for an ill and disabled patient population was unscientific and unsound, and provides a false recovery or "normal range". Technically (statisically) speaking, they used a non-representative demographic sample to determine recovery thresholds, and inappropriately used a mean and standard deviation for data that doesn’t have a normal distribution, to calculate the normal range. Averaging for sick and ill people while ignoring the original and well established, widely used markers for recovery and improvement, makes a mockery, nonsense and scandal out of this PACE trial and its supporters.
Even 75 or more on SF-36 and 4 or less on Chalder scale would have signalled improvement, but this was not used. These changes were not used for "interpretation purposes" as alleged, but to find new so called "recoveries" or those in the so called "normal range". The PACE researchers should have stuck to the original protocols for recovery and the the 3 limited (non biological) objective markers, and used them at the end, and accepted the findings, whether good or bad.
The World Health Organization (2004), A Practical Guide for Health Researchers states: “Writing the research protocol
“… once a protocol for the study has been developed and approved, and the study has started and progressed, it should be adhered to strictly and should not be changed. This is particularly important in multi-centre studies. Violations of the protocol can discredit the whole study…”
(http://whqlibdoc.who.int/emro/2004/9290213639.pdf)
The Research Councils UK Policy and Code of Conduct on the Governance of Good Research Conduct states:
“All research should be conducted to the highest levels of integrity, including appropriate research design and frameworks, to ensure that findings are robust and defensible. [] This code therefore concentrates on entirely unacceptable types of research conduct. Individuals involved in research must not commit any of the acts of research misconduct specified in this code.”
“Falsification~
This includes the inappropriate manipulation and/or selection of data, imagery and/or consents.”
“Misrepresentation, including: misrepresentation of data, for example suppression of relevant findings and/or data, or knowingly, recklessly or by gross negligence, presenting a flawed interpretation of data;” (http://www.rcuk.ac.uk/documents/reviews/grc/goodresearchconductcode.pdf)
The Medical Research Council (MRC) Guidelines for Good Clinical Practice in Clinical Trials states: “2.5 Clinical trials should be scientifically sound and described in a clear detailed protocol.
2.6 A trial should be conducted in compliance with the protocol that has received prior Ethical Committee favourable opinion.”
(https://www.mrc.ac.uk/documents/pdf/good-clinical-practice-in-clinical-trials/)
The new mean (average) figure did not give details about individuals which would be necessary for identifying the failures and successes at individual level and analysing these, and then drawing up new statistics and analysis from this.
Although the study authors said that they changed the recovery criteria before the analysis, the use of the “normal ranges” suggests that the changes were made after the study’s general results were known. This goes against the principles and ethics of scientific trials.
The 6 minute walking test was proposed by PACE researchers as “an objective measure of physical capacity” and improvement / recovery but it did not support alleged treatment success and recoveries. A third of those in the exercise section who finished other aspects of the trial never completed the final walking test. In subsequent comments in a science journal, the PACE investigators dismissed the walking-test results as irrelevant, non-objective and fraught with limitations. An extraordinary change of mind and direction. PACE researchers asked participants to wear the actometers only at the beginning of the trial, but not at the end ; thus making an accurate assessment imposssible. There was a slight increase in state benefits / insurance benefits received by patients which breached on of the trial's objectives. (If the trial had been successful, and significant numbers of people restored to normal health, they would have gone off benefits and looked for or taken up full time work or education). All the objective measures in PACE, presented in journals - 6 minute walking test, step test, and data on employment and the receipt of financial information failed to demonstrate recovery.
What Illness or Illnesses ?
They used the Oxford Criteria, London Criteria and CDC criteria which already have been found to be inaccurate and outdated and lacked diagnostic biomarkers (4,5,7). Only 67% met the CDC criteria, 100% met the Oxford criteria, and only 51% met the London Criteria. This strongly suggests that people with other illneses were recruited into the trial. The term Chronic Fatigue Syndrome (CFS) emerged from the Lake Tahoe epidemic in the USA and the response of the Holmes Committee of the CDC in 1987-88. This defintion of CFS was based on the Lake Tahoe epidemic findings. It included biological findings involving the immune system, physical reactions to infection, muscular and endocrine abnormalities. The Oxford defintion of CFS was invented by psychiatrists in 1991 and had obvious psychiatric bias. It rejected and ignored the Lake Tahoe epidemic findings and the CDC's findings, and all immune system findings, viral and pathogen findings, brain and neurological findings, mitochondria findings and endorcine findings, and all objective markers. The Oxford CFS criteria presented a subjective, quite simple and biased psychiatric explanation of the illness, which has proved inadequate, ineffective, unscientific and possibly harmful. The NIH in the USA and many medical doctors in countries reject the Oxford critera.
The London criteria have never been published and are not available as a reference for identification. They were mentioned in the National Task Force Report in 1994 as being one of nine different proposed definitions and descriptions.
The London criteria have never been used in research (before criteria can be used in research, they need to be submitted for peer review and published in an accessible form).
The London criteria have not even been consistently defined – there are different versions of them and a definitive version has not been identified.
The authors of the London criteria remain to be established as there are divergent claims about who the authors might be.
The Oxford criteria focuses on fatigue and psychiatry, the London criteria focuses on post exercise malaise not fatigue, and the CDC criteria focuses on fatigue combined with biological factors. This created contradictions and conflicts between the criteria used.
The CDC criteria, and to a greater extent the Oxford Criteria and London critera are inexact and imprecise, and would have recruited patients with other illnesses including mental illnesses, as confirmed by studies by Jason et al. and Bested et al.
47% of PACE trial participants had a co-morbid psychiatric condition at randomization. Yet the CDC criteria excludes patients with a psychiatric condition
The PACE trial most likely recruited many people who did not have ME, but other illneses, including mental illnesses which may or may not respond moderately to GET and CBT, depending on the mental illness. The inaccurate and inadequate diagnostic criteria used to recruit people, the use of purely psychiatric diagnostic criteria such as Oxford criteria and conflicting criteria to recruit people, the lack of biological data and biomarkers to confirm genuine ME and CFS cases, the unblinded trial, and the subjective outcomes and lack of objective biological evidence based outcomes were all serious flaws.
Importantly, the biomarkers for the biological abnormalities, dysfunctions and infections present in ME patients were not diagnosed and measured at the start, during and at the conclusion of the trial, and they ignored the Canadian Consensus Criteria (2003). Some known biomarkers mentioned on www.me-ireland.com/scientifc.htm . So an ME or CFS patient couild be ill with biological abnormalities and dysfunctions and chronic infection(s) but this was conveniently ignored and dismissed by psychiatrists running the PACE trial. This combination of no biomarkers and no biological evidence combined with a refusal to accept the Canadian Consensus Criteria (2003) means there is a high probability that most of these patients did not have ME. Severe ME patients were deliberately not recruited. This in iself is very revealing as research shows that severe ME patients are usually not recruited for CBT and GET trials and treatments. (Chambers D, Bagnall AM, Hempel S, Forbes C (2006). "Interventions for the treatment, management and rehabilitation of patients with chronic fatigue syndrome/myalgic encephalomyelitis: an updated systematic review". Journal of the Royal Society of Medicine 99 (10): 506–20.). Severe ME cases would have disproved the claims and presumptions made by psychiatrists about CBT and GET. Because of flaws in the design and recruitment of the trial, many of these patients did not have ME. So the question is - what illnesses did they have ? which patients are they referring to when making claims of "recovery" and "improvement" ?
They did not subgroup patients according to neurological, endocrine, PEM, infections, illness severity and immune system factors.
The trial had no properly matched control group, and it was unblinded, outcomes or results were subjective not objective. The limited objective tests were unsuccessful in terms of recovery, and were discarded and dismissed as irrelevant at the end of the trial. This is discused in more detail below.
the "English adult population" study they used for the original recovery criteria failed to screen for old age factors, underlying illnesses, diseases and disabilities, physical and intellectual impairments, obesity, total sugar and fat intake, alcoholism, and lifestyle and stress factors in such supposedly "normal" populations. The working age population in good health was not included as the main marker, the criteria. This is a serious error and undermines the reason for revising the primary outcome criteria. And in addition to this error, the bar for "recovery" was then set too low in this trial, and as a result, ill people could be termed "recovered". There has been an accumulation of errors in this trial.
"Recovery"
In 2016, following several Freedom of Information requests and a court order, the PACE researchers finally releasd the PACE data to the general public. The data showed that recovery as defined in the original published protocol was:
3.1% for specialist medical care alone (SMC)
6.8% for cognitive behavioural therapy (CBT)
4.4% for graded exercise therapy (GET)
1.9% for adaptive pacing therapy (APT)
Source: A preliminary analysis of 'recovery' from chronic fatigue syndrome in the PACE trial using individual participant data. Alem Matthees, Tom Kindlon, Carly Maryhew, Philip Stark, Bruce Levin.21 September 2016 http://www.virology.ws/wp-content/uploads/2016/09/preliminary-analysis.pdf
These figures show that the PACE trial was a failure. In fact the results were less than what one would get from a placebo. In 2013, the PACE researchers had wrongly claimed that CBT led to "recovery" in 22%, GET led to "recovery" in 22%, APT led to "recovery" in 8% and SMC led to "recovery" in 7%. These figures were wrong and over inflated. These figures were also wrong and over inflated. These figures are also discredited by the many flaws and defects in the PACE trial. The improvement itself was subjective, and open to interpretation, and was not supported by objective evidence proposed by the original PACE protocols, and other objective evidence in the form of biological markers. This lack of evidence was worsened by the fact that the markers for "recovery" were changed towards the end of the trial. Furthermore what illness did this tiny number of people recover from ? the diagnostic criteria for the trial was flawed and accepted some people who did not have ME / CFS, but had other illnesses. All of these factors combine together to bring the PACE trial and its findings into disrepute and make them unacceptable in a medical and scientific context.
A 30% recovery rate was cited in the Lancet but was later retracted as it was found to be wrong and misleading.
Half of participants in the standard medical care (SMC) group rated it as not being a logical treatment for them and only 41% were confident about being helped by specialist medical care. (Sharpe, M, Goldsmith, KA, Johnson, AL, Chalder, T, Walker, J, and White, PD. Rehabilitative treatments for chronic fatigue syndrome: long-term follow-up from the PACE trial. Lancet Psychiatry. 2015; 2: 1067–1074).
The standard medical care (SMC) did not involve intensive and comprehensive medical diagnostics and lab tests to identify the biological abnormalities and dysfunctions present and any chronic infections present. Ignoring these biological factors undermined the doctors and the medical treatments given. It was incapable of delivering high quality, accurate treatments. It is no surprise that it's results were similar to CBT and GET, which were disappointing and ineffective. The standard medical care was flawed from a scientific and medical perspective, and cannot be compared or contrasted with any other type of treatment.
In 2015, the PACE results show that the overall mean short-form 36 (SF-63) physical functioning score is less than 60. This means most patients are still very ill and disabled. Lupus has a mean score of 63, congestive heart failure has a mean score of 60 while healthy individuals with no illness have a mean score of 93. This means the PACE trial was a failure and that CBT and GET are ineffective. We will also analyse the harms caused by CBT and GET in sections below.
In 2015, the PACE trial follow-up study concluded that outcomes with standard medical care (SMC) alone or adaptive pacing therapy (APT) were similar to CBT and GET at follow-up. (Sharpe, M, Goldsmith, KA, Johnson, AL, Chalder, T, Walker, K, and White, PD. Rehabilitative treatments for chronic fatigue syndrome: long-term follow-up from the PACE trial. Lancet Psychiatry. 2015; 2: 1067–1074)
CBT and GET were no different to receiving no treatment.
the PACE researchers did not state what "recovery" actually meant - did the patients resume full time work ? did they apply for full time work and attend interviews for jobs ? did they go off disability payments and register as being fit for work and available for work with the social welfare and other government departments ? did they feel ready to resume full time work ? were they capable of working 8 - 9 hours a day, 5 days per week ? can they rise early in the morning 7 - 8 am to attend work or training ? was there a return to full health and can this be conclusively proved scientifically and medically ? did they recover the full exercise capabilities of a healthy able bodied person ? did they return to sporting activities ? did they engage in full social activities, dating and relationships, and educational activities of a normal healthy person ?
The PACE researchers have not published details of this in medical and scientific journals.
the missing data in the trial relating to 33 people is ominous and this further undermines it's credibility. The PACE investigators failed to provide adequate security for patient information and files.
will these so called "recoveries" be consistent over 2 - 10 years ? This is important considering the fact that CBT and GET benefits, if any, do not last more than 1 year (8) .
In 2013 and 2015, information on PACE trial details and results were requested by researchers under the Freedom of Information Act in Britain. This request was denied by a tribunal in one case and denied by University authorities in another case, which was very unusual and unexpected. The researchers sought more detailed results including data on patients who deteriorated and worsened after the PACE trial.
Since 2011, PACE authors have tried to block all requests for information about the PACE trial under the Freedom of Information act in Britain. This blocking of data is vexatious to other scientific researchers, medical doctors and patients. And is creating a vexatious relationship between the PACE researchers and other parties. Why yhe blocking and refusals, are the PACE authors covering up ? have they something to hide ? This goes against scientific principles of transparency, openness, opportunities for replication and verification, and integrity and honesty.
The Declaration of Helsinki states: “36. Researchers, authors, sponsors, editors and publishers all have ethical obligations with regard to the publication and dissemination of the results of research. Researchers have a duty to make publicly available the results of their research on human subjects and are accountable for the completeness and accuracy of their reports.”
They did not publish how many patients recovered and worsened according to the original 4 recovery criteria and the 3 objective criteria at the start if the PACE trial. And did not give independent researchers full access to the raw data
They did not publish how many people dropped out of CBT and GET treatments on the PACE trial
They did not publish how many people got worse from CBT and GET treatments on the PACE trial
The PACE trial did not address the
the harm which exercise does to ME patients, and did not acknowledge the existence of Post Exertional Malaise, Systemic Exertion Intolerance Disease (SEID) and Post Exercise Neuo Immune Exhausation (PENE). I refer PACE authors to the research and clinical findings on this at www.me-ireland.com/scientific/16.htm
in ME and CFS, which can be adversely affected by exercise.
"A review involving patients with cancer or chemotherapyinduced fatigue referenced four studies where oxidative stress was held to be the cause of severe fatigue experienced by patients in those studies [99]. Elevated O&NS is also causatively implicated in the development of severe central or “systemic” fatigue [100–103]. A recent review highlighted seven studies where authors cited a significant positive association between oxidative stress and severity of fatigue in patients diagnosed with CFS [5]. Oxidative stress is dramatically elevated in patients with CFS compared to healthy controls during the conduct and aftermath of exercise [104, 105]." Source: The Neuro-Immune Pathophysiology of Central and Peripheral Fatigue in Systemic Immune-Inflammatory and Neuro-Immune Diseases Morris et al. 2015.
The PACE authors did not track the damaging effects of exercise on dysfunctional mitochondria, heart, circulation, muscles, brain and nervous system, immune system, blood vessels and other body systems in ME patients
Some of the PACE researchers and their supporters called ME and CFS imaginary illnesses, "all in the mind", psychological illnesses, psychosomatic, and "non illness" in the past, and ridiculed and insulted such patients ; some facts are presented here at www.ireland.com/bogus.htm . Some may try to deny this, but their past quotations in public and in papers and correpsondence reveal the facts and truth. Should these type of people be carrying out PACE trials or analysing them and supporting them in public ?
The six centers around England participating in the PACE trial applied different methods for assessing safety. This raises questions about lack of standarisation, lack of consistency, and how to interpret the results, and whether the overall claims of “safety” can be taken at face value.
Conflicts of Interest
Some of the PACE trial leaders had undeclared conflicts of interest, including previous work for the private insurance industry where they classified ME as being a psychiatric disorder, requiring CBT and GET, and ME patients were refused disability benefits and refused lab tests. These PACE researchers made large amounts of money from this work in the past, and expected to continue doing so once the PACE trial findings were published. They continue to have strong links with the insurance industry, and they had a vested interest in obtaining a certain outcome in the PACE trial. The patients in the PACE trial were not informed about this. Some further information about these conflicts of interest are provided here.
One PACE researcher had an undeclared conflict of interest in relation to a newsletter shown to PACE participants which endorsed and praised CBT and GET, using the U.K. clinical guidelines committee and 'independent' testimonials from participants in the PACE trial. She served on the U.K. clinical guidelines committee in the past and the PACE research team and was using the newsletter to promote her previous work for the U.K. clinical guidelines committee. The use of the newsletter in the PACE trial had the effect of influencing how patients viewed the PACE treatments offered. No mention was made of adverse outcomes using CBT and GET and the lack of full recoveries and there was no mention of biological abnormalities and of biological diagnostics and treatments. This brought bias and a placebo effect into the PACE trial. The patients in the PACE trial were not informed about this. Trying to influence and manipulate trial participants (patients) in a certain way in a trial which is unblinded and has subjective outcomes and results is a serious breach of Ethics.
The power of suggestion was cynically used by researchers in a Newsletter given to trial participants to downplay harms, deterioration, and a worsening of symptoms, while encouraging feelings of improvement and feeling better. There was a high risk a 'stockholm syndrome' scenario. The lack of objective markers, blinded trials, placebos, and the use of subjective markers and results which can be skewed by the power of suggestion further undermines the validity of the PACE trial.
The PACE authors claimed that CBT and GET were cost effective to society, but how is it cost effective to keep patients sick and ill for years and decades ? It is estimated that ME costs the US economy over $20 billion per year and imposes similar costs on other countries. It imposes a massive financial burden on health systems, social welfare systems, health insurance systems, businesses, economies, individuals, families, and home care. This financial burden is worsened by the fact that CBT and GET are ineffective and useless in treating complex biological illnesses such as ME, and this imposes a continuous cost and serious financial burden to the aforementioned parties. And constitutes a gross neglect of patients.
Letters to the Lancet and CDC authored by medical doctors and researchers
Dr. James C. Coyne, is Professor of Health Psychology at University Medical Center, Groningen, the Netherlands. He is also Visiting Professor, Institute for Health, Health Care Policy & Aging Research, Rutgers, the State University of New Jersey. Dr. Coyne is Emeritus Professor of Psychology in Psychiatry, where he was also Director of Behavioral Oncology, Abramson Cancer Center and Senior Fellow Leonard Davis Institute of Health Economics. .He gave a very informative lecture about the PACE trial in Edinburgh in 2015.
Professor James Coyne also run a Blog about the PACE trial, which raises points of scientific and medical interest
It was stated to patients in the trial that patient data would be kept secure, but this was not followed, and some patient data went missing, and some was stolen. This breaches the rules and ethics of scientific trials. This is also a case of criminal negligence.
they did not state what beneficial effects GET and CBT would have on the chronic viral and pathogen infections, immune system dysfunctions, autoimmunity factors, HPA axis dysfunctions, Neurological dysfunctions and deficits, mitochondria and krebs cycle abnormalities, methylation cycle blocks, post exercise malaise (PEM), orthostatic intolerance and Postural Tachycardia Syndrome, cardiac abnormalities, etc, consistently found in ME patients. The reason being that CBT and GET cannot treat these medical / biological abnormalities in ME patients.
Wessely school psychiatrists have admitted in the past that CBT and GET cannot cure ME and that the alleged " benefits" are temporary (8). Then why did they waste millions of pounds of British taxpayers money on the PACE trial ?
Dr. White who ran the PACE trial previously published a few studies showing increased cytokine abnormalities and inflammation in ME patients after exercise. Yet he did not bother to measure these markers in the PACE trial, and he did not include them in baseline measurements or outcome measurements. He showed a disregard for his own biological findings in the past. This showed a disregard for scientific method, scientific rigour and for patient safety.
The trial did not produce any objective scientific evidence such as changes in biomarkers and biological markers over time to track and verify these so called "improvements" and "recoveries", and deterioration and relapses.
International Petition by ME and CFS patients asking the CDC and HHS in the USA to independently investigate the PACE trial and remove all references to PACE trial, CBT and GET in treatments for ME, CFS or SEID.
Some recent research into CBT, GET and Pacing in Britain in 2015 contradicts the PACE findings. Of patients who received GET, 74 percent said that it had made them worse. While 18 percent said they were worse after cognitive behavior therapy and only 14 percent after pacing
.
In 2017, the CDC in the USA removed GET and CBT from the section of their web site dealing with ME and CFS. They are responding to growing evidence that CBT and GET are not proper treamtents for ME / CFS and no not bring aobut recovery.
The PACE trial and results are discredited, meaningless, and useless in a scientific context and medical context. It is also wasteful of government funds and private funds.
Other psychiatrists have claimed that cognitive behavior therapy and exercise therapy had a beneficial effect in their "ME trials" - for whom ? their psychiatric patients or those with diseases other than ME ? Their scientific "trials" had no full recoveries from ME and nobody was able to return to full time work and resume a normal working life and social life and recover the full exercise capabilities of a normal healthy person. Furthermore, they did not test for bio-markers for each of the abnormalities and dysfunctions present in ME and other objective data prior to, during and after these tests, in order to establish progress and recovery, and they did not continue this for 12 months, 24 months, 36 months to measure efficacy, safety and overall effectiveness. And they ignored all the biological and biomedical evidence that exercise can be damaging to ME patients, and ignored the relapses and worsening of symptoms from exercise in ME (6). Furthermore they consistently ignored the scientific and medical evidence that ME is a serious physical biomedical illness as shown by over 5,000 research papers. These trials tend to be sloppy, badly designed, inaccurately recruited, unethical and have far too much psychiatric bias and they should be retracted and rejected by scientific journals.
Criminal Aspects
It is a criminal offence to cause harm and /or financial damage to another person(s). It is also a criminal offence in Britain (and many other countries) to aid and abet or support in any way a person(s) involved in criminal activity. Criminal charges and civil damages charges could be taken against certain psychiatrists, insurance companies and medical doctors. The dismissal and ignoring of all biological research into ME / CFS in over 5000 research papers, and of known biological markers, while accepting false psychiatric claims has had dire consequences for patients, ranging from terrible suffering and deterioration for many years, financial losses, break up of family and relationships, and premature deaths. The high number of deaths from ME / CFS and the enormous suffering inflicted on many patients over many years through medical neglect borne of dismissal of the disease as a psychiatric illness by medical authorities, represents criminal neglect, assault, grevious bodily harm, and may constitute manslaughter in certain cases. The harms caused by CBT and GET treatments constitute criminal acts, ranging from assault, grevious bodily harm, criminal negligence, to manslaughter. The failure to inform patients of these harms and risks represents medical negligence and the breach of the law concerning consent. Refusals of insurance companies to pay benefits to ME / CFS patients can be prosecuted in criminal courts under fraud, breach of contract, and RICO charges and sued in civil damages courts. In the USA RICO charges and suing for benefits and other costs have been successfully undertaken by patients. Insurance companies or doctors which recommend CBT and GET as treatments for ME / CFS may be financially liable for the harms caused and financial losses endured.
The denial of adequate medical diagnostics and treatments to ill people by governments is a breach of human rights, common law rights and Constitutional rights, and can have criminal consequences and civil damages consequences. The denial of or misdirection of government funds for biological research into ME / CFS - a denial which was orchestrated by certain influential psychiatrists meant patients were deprived of vital biological research which would provide more accurate and effective diagnostics and treatments, and this had the effect of prolonging the suffering and deterioration of patients, and causing premature deaths ; there are further criminal offences here. The conflicts of interest in research, advice given to government and government bodies, advice and guidelines given to medical doctors and medical bodies, and advice and services offered to insurance companies and the enrichment of some psychiatrists while patients were neglected, suffered and died prematurely includes more criminal offences.
Exposing Bogus Treatments and Research Claims & Defending the Legal and Human Rights of ME & CFS patients in an Environment of Deceptions, Fraud, Neglect, Abuse, Insults and Social Stigma
Are ME and CFS patients entitled to be treated with respect ? do they have rights ? this is a very important question. It determines the quality of one's life and one's lifespan. Respect is the foundation of your life, your rights, your being, your existence, and if you don’t have that, then you have nothing. The very nature of the false psychiatric claims about ME and CFS have destroyed this respect, let us examine this issue:
The denial of internationally agreed and peer reviewed medical, biological based diagnostics, biological lab tests (based on aforementioned diagnostics and known biomarkers and scientific research findings) and treatments based on these to ill people by governments or insurance companies is a breach of human rights, common law rights and Constitutional rights, and can have criminal consequences and civil damages consequences.
the denial of proper medications for ME and the neglect of patients by doctors and medical authorities, and the incredible suffering of severe ME patients, and the many deaths from the illness ( http://www.ncf-net.org/memorial.htm) . Causing the death of others is a criminal offence and there are also civil damages and tort liabilities.
the deliberate refusal of governments and academia to fund biological research into the illness and the under funding of biological research into the illness for the last 20 years in several countries. It received far less funding than similar illnesses with similar demographics and economic losses ( 100 - 120 times less). This is analysed on www.me-ireland.com/research2.htm . This lack of funding and under funding was directly related to psychiatric bias, the "all in your head" prejudices. In Britain, this under funding was orchestrated by some British psychiatrists who have considerable influence at government levels and also internationally.
the manipulation and abuse of medical bodies and doctors to propagate a false psychiatric agenda
the ineffective, inadequate and unsafe CBT and GET treatments for 24 long years while biological findings and lab tests are refused
the false imprisonment of Karina Hansen in Denmark and false imprisonment of others in the past
the legal threats and professional threats to doctors, professors, researchers and journalists by certain psychiatrists
the refusal to acknowledge biomarkers and carry out lab tests to identify biological abnormalities
the refusal to publish biological findings and letters in top medical and scientific journals
the refusal of some psychiatrists to release research data under the Freedom of Information act
the "psychiatric" social stigma attached to ME and CFS, and accompanying abuse and harassment of patients in society as a result of false psychiatric viewpoints
about the disease
the loss of earnings and career for patients from medical neglect and psychiatric nonsense
the insulting and abusive comments of many doctors and psychiatrists
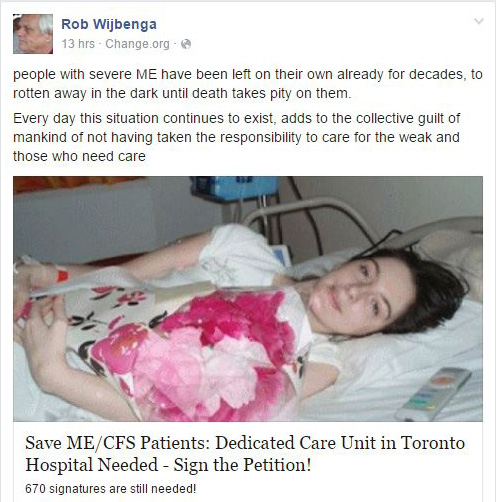
These clearly show an appalling lack of respect for ME and CFS patients. The following Facebook message and petition by an ME/CFS advocate outlines the problem faced by many patients, particularly severe ME cases
ill ME / CFS patient being
taken to hospital. Ineffective treatments like CBT and CET cannot
improve or cure ME / CFS
What can be done ? what has been done ? being quiet, patient, placid, cowardly, submissive, and waiting and waiting has not solved this problem. In fact it has made it worse. All of the factors mentioned above concerning disrespect, neglect and abuse of patients continue to exist. Should ME and CFS patients be content with this ?
There are solutions, legal solutions which assert your legal rights, your common law rights, your human rights and your Constitutional rights. These will involve court cases, judicial reviews, appeals, tribunals, parliamentary questions, political lobbying, parliamentary committee hearings, and expert panel hearings, solicitor’s letters to doctors, medical bodies, insurance bodies, politicians and civil servants, and various other type of court and tribunal actions to enforce your rights and enforce respect. The IOM took ME and CFS very seriously when Mrs. Burmeister used various legal actions and threats to assert her rights and the rights of all ME / CFS patients. And insurance companies and drug companies respected ME/CFS when they were brought to court and had to fight in courts. Let us examine how you can bring legal actions to assert your rights and dignity and get justice.
Basis for Legal cases and Court cases
Medical negligence, neglect and malpractise. The denial of internationally agreed and peer reviewed medical, biological based diagnostics, biological lab tests (based on aforementioned diagnostics and known biomarkers and scientific research findings) and treatments based on these to ill and disabled people by governments or insurance companies is a breach of human rights, common law rights and Constitutional rights, and can have criminal consequences and civil damages consequences in terms of prolonged suffering, deterioation of health and deaths.
Misdiagnosis - failing to or refusing to properly test for Chronic Lyme or other diseases similar to or co-existing with ME / CFS . Negative results using old and outdated equipment and methodologies which are contradicted by the patient accessing more accurate and precise tests elsewhere which give positive results have legal consequences in terms of damage to the patient's health in terms of misdiagnosis.
Deliberately ingoring and covering up accurate diagnostics, denying patients access to these diagnostics, and keeping patients ill for long periods
of time causing significant pain, physical injury to patients and loss of earnings
Patient deaths from ME / CFS resulting from (i) the dismissal and ignoring of all biological research into ME / CFS in over 5000 research papers, and of known biological markers (ii) refusal to use internationally agreed and peer reviewed medical diagnostics and lab tests while accepting false psychiatric claims, all of which has had dire consequences for patients, ranging from terrible suffering and deterioration for many years, financial losses, break up of family and relationships, and premature deaths. The high number of deaths from ME / CFS and the enormous suffering inflicted on many patients over many years through medical neglect borne of dismissal of the disease as a psychiatric illness by medical authorities, represents criminal neglect, assault, grevious bodily harm, misdiagnosis, malpractise, and may constitute manslaughter and murder in certain cases.
Loss of earnings and assets for patients resulting from medical negligence, malpractise and denial of accurate diagnostics and treatments
Get High court Orders of Performance to enforce proper diagnostics and treatments for ME, CFS, Fibromyalgia and Chronic Lyme disease
ME and CFS patients and organisations joining together nationally and getting solicitors and barristers to send letters and issuing court proceedings against government health bodies (HSE in Ireland, NHS in Britain, DHHS in USA, etc.) and national medical organisations to implement and enforce internationally agreed and peer reviewed medical, biological based diagnostics, biological lab tests (based on aforementioned diagnostics and known biomarkers and scientific research findings), and biological based treatments for ME and CFS.
Court orders of performance to enforce the aforementioned medical diagnostics and treatments for ME / CFS
Refusals of insurance companies to pay benefits to ME / CFS patients can be prosecuted under fraud, breach of contract, and RICO charges and sued in civil damages courts.
Failure of medical doctor(s) to tell patient about risks and harms from CBT and GET when prescribing them. And failure to tell patient about ineffectiveness of CBT and GET in terms of recovery. It is a criminal offence to cause harm and /or financial damage to another person(s). It is also a criminal offence in Britain (and many other countries) to aid and abet or support in any way a person(s) involved in criminal activity.
Failure of medical doctor(s) to tell patient about any reasonable alternative or variant treatments. This would include anti viral treatments, immune system treatments, etc. as successfully used by other medical doctors, please read www.me-ireland.com/diag-treat.htm. For example, there was a randomized clinical trial(by Dr. Montoya in California) showing the benefits of the antiviral Valcyte (valganciclovir) for ME/CFS, it could be argued that your doctor is under a duty to inform you of the possible benefits (and risks) of Valcyte treatment.
Use of case law and legal precedents in relations to ME and CFS and other illnesses and disabilities
The denial of or misdirection or misappropriation of government funds for biological research into ME / CFS has denied patients of necessary resarch into the disease. This defrauds the taxpayers, the government and ill patients and is a breach of the law.
Medical doctors or psychiatrists mocking, belittling, insulting, slandering ME / CFS patients with the result that these patients are denied proper treatments and suffer continuing illness and physical injury is a breach of medical guidelines and ethics and a breach of a patient's rights and the law
The decisions of the Norwegian government, Canadian government, Australian government, and Japanese government to accept biological based diagnostics for this disease
The ignorance and negligence of those persons operating Blood Banks and Blood Transfusions and the continued infection and re-infection of the general population
the alleged right to privacy being used by PACE researchers to refuse release of research data is fallacious and misleading. Privacy can be preserved through total annonymity making it possible to hide their names, age, sex, doctor, place of origin / residence and other personal details. This was applied in the FINE trials and other similar trials. Under the Freedom of Information act the right to protect annonymity must be weighed with other factors such as furthering the progress of science, the protection of patient lives through identifying harms and risks, and identifying ineffective treatments which could increase the risk of neglect and premature deaths.
Here are some no win, no fee medical negligence solicitors in the UK:
Legal Facts - Serious Physical, Biological Illnesswhich has caused Deaths
The potent combination of immune system dysfunctions and chronic infection(s), mitochondria and Krebs cycle malfunction, Neurological dysfunctions, Cardiac and vascular damage, increased risk for certain Cancers, Endocrine and HPA axis dysfunction and high levels of oxidative and nitrosative stress cause a patient to deteriorate physically and become very exhausted and weak over time. Many ME sufferers end up bed-ridden, house bound or in wheelchairs. ME can be deadly, thousands of people around the world have died of ME and health complications caused by ME , see Memorial section. New research into causes of death in ME presents a very disturbing picture, click here to view findings - Patient deaths from ME . Comedians like Ricky Gervais have made fun of and mocked and laughed at such disabled people, and this is despicable, perverted, and disgraceful. There should be standards, ethics and laws in the entertainment industry to strongly discourage / punish such behaviour.
ME bears a resemblance to Cancer and AIDS in the sense that many ME patients have died of opportunistic infections, heart failure and certain cancers due to a depleted immune system and high levels of oxidative stress (and it's effects). Research has recently shown that most ME patients have serious heart and vascular abnormalities arising from ME itself, making them highly susceptible to a sudden heart attack. There is also a high rate of suicide among ME patients, this being brought about by frustration, desperation for some cure, social isolation, lack of proper medical care, no support, constant pain, exhaustion and weakness, and financial hardships.
On 15th October 2009, Professor Nancy Klimas, then Professor of Medicine, Microbiology and Immunology at the University of Miami, famously said in the New York Times: “I hope you are not saying that (ME)CFS patients are not as ill as HIV patients. I split my clinical time between the two illnesses, and I can tell you that if I had to choose between the two illnesses I would rather have HIV”. Dr. Nancy Klimas, is an internationally respected doctor and Immunologist and an expert in both ME / CFS and AIDS.
"There is evidence that the patients with this illness experience a level of disability that is equal to
that of patients with late
-
stage AIDS, patients undergoing chemotherapy (and) patients with
multiple sclerosis" Professor Nancy Klimas, University of Miami, speaking at the launch of the US
CDC campaign to raise awareness of ME/CFS, 3 November 2006, National Press Club, Wa
shington
DC
In 1995, Professor Mark Loveless, Head of the AIDS and ME/CFS Clinic at Oregon Health Sciences University said in his US Congressional Briefing that an ME/CFS patient: “feels effectively the same every day as an AIDS patient feels two weeks before death; the only difference is that the symptoms can go on for never-ending decades”. Mr. Loveless supported his statement with data from research conducted at his own institution and morididity data provided by other ME experts who had compared the two diseases (AIDS and ME ).
In 1994, Dr. Anthony Komaroff of Harvard Medical School reported that the brains of those people with ME/CFS were identical to those with AIDS dementia, when viewed with SPECT imaging. They were both completely different to normal healthy brains. He believed that ME/CFS cases were the result of viral infection of the brain and nervous system, similar to AIDS.
SPECT imaging of the brain: comparison of findings in patients with chronic fatigue syndrome, AIDS dementia complex, and major unipolar depression.
Schwartz R , Komaroff AL, Garada BM, Gleit M, Doolittle TH, Bates DW, Vasile RG, Holman BL. AJR Am J Roentgenol. 1994 Apr;162(4):943-51.
In 1994, one of the world’s most renowned ME/CFS clinicians, Dr Daniel L Peterson from the US, went on record: “In my experience, it is one of the most disabling diseases that I care for, far exceeding HIV disease except for the terminal stages” (Introduction to Research and Clinical Conference, Fort Lauderdale, Florida, October 1994; published in JCFS 1995:1:3-4:123-125).
In September 2012, Dr Sandra Kweder of the FDA in America called ME/CFS "a serious or life threatening disease".
In 2004, Dr William Reeves, Chief of the ME/CFS research programme at the US Centres for Disease Control, (CDC) reported that ME/CFS patients “are more sick and have greater disability than patients with chronic obstructive lung or cardiac disease, and that psychological factors played no role” (Press Release, AACFS, 7th October 2004).
Also in 2004, a randomised clinical trial found “In comparison with other chronic illnesses such as multiple sclerosis, end-stage renal disease and heart disease, patients with (ME)CFS show markedly higher levels of disability” (Am J Occup Ther 2004:58:35-43).
In 1990, Dr. Nancy Klimas published a research paper in the Journal of Clinical Microbiology, in it she reported that the array of immunological defects in ME suggests that it is a form of acquired immuno-deficiency (Nancy Klimas, et al "Immunologic abnormalities in Chronic Fatigue Syndrome", Journal of Cliniucal Microbiology, 28, (June 1990) )
Dr. Paul Cheney (who has successfully treated hundreds of ME patients) stated "These patients look a lot more like multiple sclerosis (MS) patients or AIDS dementia patients, whose dysfunctions are also subcortical".
On the Sickness Impact Profile Scale (SIPS), ME patients test as high or higher than people with Cancer and heart attack (Oslers Web, by Hillary Johnson, Penguin Books 1997, page 292).
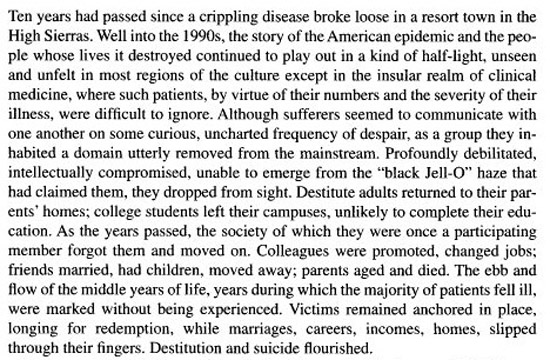
The following passage from the book 'Osler's Web' by Hillary Johnson depicts the devastating effect of ME on people
What Evidence ?
1. Research for Legal Use in Courts Listing of Research findings and papers worldwide and categorisation of biological abnormalities and dysfunctions and infections found in ME. This proves it is a physical and biological illness and not a psychiatric illness or psyhciatric disorder.
The following paper by the organisation Paradigm Change details many of the biological abnormalities, dysfunctions and infections found in ME and CFS patients and research papers to support this. ME/CFS and Medical Abnormalities - Medical Research paper.
After 1990, new bogus diagnostic criteria (Oxford criteria) and non treatment and neglect of patients was introduced by a minority of psychiatrists and this failed patients, leaving most in a state of severe illness for several years and decades, destroying the lives of many ME patients and their families worldwide and leading to many deaths, see http://www.ncf-net.org/memorial.htm
2. Diagnostic and Treatment Protocols and Biological based medical clinics
3. Historical Legal Facts for Legal Use ME (CFS) has been accepted as a physical, biological or organic illness from 1955 to the present day by medical authorities and doctors worldwide. But after 1990 there were attempts by a minority of psychiatrists to classify it as a psychological illness and ignore and dismiss the findings of doctors, scientists and medical authorities since 1955.
Myalgic Encephalomyelitis or ME was first used to define the illness by Dr. Donald Acheson in the Lancet medical journal in 1955 and has been used ever since - Outbreak at the Royal Free.
E.D Acheson. The Lancet, Volume 266, Issue 6886, Pages 394 - 395, 20 August 1955.
After 1955, Dr. Acheson's paper was followed by an article in the Lancet by Sigurdsson describing the illness and it's history A new Clinical Entity ? in 1956. In that same year, a paper by Dr. Melvin Ramsay appeared in the Lancet Encephalomyelitis simulating Poliomyelitis . Dr. Melvin Ramsay was a consultant physician at the Infectious Diseases Department of the Royal Free Hospital, and he also served as advisor to the Ministry of Health in matters concerning smallpox. He was actively involved in treating ME patients during the Royal Free Hospital outbreak. He went on to become a leading global expert in ME, spending 35 years diagnosing, treating and researching ME, and other diseases. There was another paper by Dr. Acheson in the Lancet in 1957 Benign myalgic encephalomyelitis followed by an article in the British Medical Journal titled 'Epidemic Myalgic Encephalomyelitis' in 1957. The ME outbreak at the Royal Free Hospital in Britain continued to interest doctors and researchers as evidenced by the paper An Outbreak of Encephalomyelitis in the Royal Free Hospital Group, London, in 1955 by THE MEDICAL STAFF OF THE ROYAL FREEHOSPITAL in British Medical Journal in 1957.And another paper that year Epidemiological aspects of an outbreak of encephalomyelitis at the Royal Free Hospital, London, in the summer of 1955
In 1957, a paper by an American, Dr. Shelokov , 'Epidemic Neuromyasthenia. An outbreak of poliomyelitis-like illness in student nurses' published in the New England Journal of Medicine provided details of a typical ME outbreak, which was quite new to medical science in America. That year a paper was published in the New England Journal of Medicine about the Punta Gorda outbreak. Another paper in 1958 shed more light on the illness - Benign myalgic encephalomyelitis. Galpine, J.F. Brit. J. Clin. Practice, 12:
186, 1958. This was followed by another more detailed paper by Dr. Acheson in the American Journal of Medicine in 1959, The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromyasthenia.n 1959 a paper appeared in the New England Journal of Medicine titled 'Epidemic Neuromyasthenia — Clinical Syndrome?' by Dr. Donald Henderson and Dr. Shelokov and this gave an an American perspective on the disease, ME. In 1955, Pellew and Miles (1955) in Australia reported that the infectious agent in ME patients was transferred to healthy monkeys and they died within a short time. Autopsies showed damage to nerve cells and blood vessels. A medical thesis by Dr. A.L. Wallis in Edinburgh University, 1957 shed some light on the outbreak of ME in Cumberland in the 1950's. An autopsy of a dead patient showed damage to nerve cells and blood vessels. The common consensus among doctors and researchers during the 1950's was that a virus was involved. By 1960, 'Myalgic Encephalomyelitis' (ME) was formally accepted and recognised by medical authorities worldwide, and in 1962 it began appearing in medical text books in University. Dr. Donald Acheson was convinced the illness involved a chronic infection with neurological, muscular and immunological effects and dysfunctions. Dr. Acheson later became the Chief Medical Officer in Britain and was a highly respected medical doctor and researcher.
There were further research papers and reviews produced by other leading medical doctors and researchers including Dr. Melvin Ramsay, Dr. E. O'Sullivan, Dr. Richardson, Dr. Galpin, Dr. Deisher, Dr. Parish, Dr. Shelokov, Dr. Henderson, Dr. Sigurdsson, Dr. Poskanzer, Dr. Gsell, Dr. Hill, Dr. Dowsett, Dr. Behan and others in medical and scientific journals throughout the 1950's, 1960's, 1970's and 1980's, see History of ME presented by Lisa Petrison to the CFSAC in 2014. They all concluded that an infectious disease, neurological dysfunctions, musco-skeletal dysfunctions, exhausation, mitochondria abnormalities, and severe inflammation were involved in the illness.
It's neurological aspects were considered important by the medical community, and ME was formally classified by the World Health Organisation as a neurological disorder in the International Classification of Diseases (ICD) in 1969 (ICD-8: Vol I: code 323, page 158; Vol II (Code Index) page 173).
Dr. Melvin Ramsay, a British medical doctor was a leading global authority on ME from 1955 to 1990, and his work was cited and used by doctors around the world. He believed that there was an infectious cause which led to neurological, endocrine, mitochondria and muscular abnormalities. His research paper 'Epidemic neuromyasthenia' 1955-1978'. Postgrad Med J. 1978 Nov;54(637):718-21. PMID:
746017, was a major contribution to medicine, and provided important insights into the illness in Britain over 2 decades. His classic book about ME, detailing its naming, definition and it's progression through the 1950's, 1960's and 1970's is Myalgic Encephalomyelitis and Post Viral Fatigue States: the Saga of the Royal Free Disease by Dr Melvin Ramsay. Dr. Ramsay knew and collaborated with Dr. Acheson and Dr. Richardson, throughout this period and their medical and scientific insights were very valuable and continue to have relevance today. Dr. Ramsay was the first person to create a formal definition and diagnostic criteria for the illness in 1986, which was used by doctors and researchers in Europe - Ramsey ME Definition 1986, 1988
Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME.
Dr. Erich Ryll a US doctor based in California studied ME patients from 1975 to 1994. He concluded that it involved infectious vasculitis, extreme inflammation, severe exhausation, and that an infectious disease was involved. Vasculitis involving the skin was recorded during ME outbreaks in Cumberland, Durham and North West London in Britian in 1955. This has been confirmed by later studies showing significant vascular abnormalities and damage to veins in ME patients.
ME is the correct scientific and medical name for the illness. The World Health Organisation (WHO) classification code for ME is G93.3, World Health Organisation - Classification . This is universally accepted by governments, medical associations and doctors worldwide. This puts ME in the same class as other neurological illnesses such as Multiple Sclerosis, Parkinsons, ALS, Epilepsy.
The research verifies that it is a neurological illness with immune deficiencies, endocrine abnormalities, mitochondria dysfunctions, and chronic infections in most cases.
4. Response of some Governments The recent actions of governments in Norway, Canada, Australia, and Japan in their acceptance of Canadian Consensus Critera (2003) or similar Biological based criteria (Japan) show that these governments legally accept ME / CFS as a physical illness requiring physical and biological diagnosis and treatments. This establishes a legal basis for biological based ME / CFS diagnosis and treatment and for public perceptions about the illness, which can be applied by governments and courts.
In 2011, the Norwegian Government apologised to ME patients and their families in Norway for neglecting them, and offering ineffective, useless psychiatric and psychological treatments for many years, which left them sick and in limbo. The government announced a change in direction towards biological based diagnostics and treatments and support for biological research such as the Rituximab trials in Norway. Norway's Directorate of Health Apologises for Treatment of ME Patients
In 2001, Health Canada appointed an international panel of experts in this emerging field of medicine, ME / CFS, to establish a clinical working-case definition, diagnostic guidelines, and treatment procedures. The panel released a set of guidelines in 2003 and their choice of name to describe the condition was both "myalgic encephalomyelitis" and "chronic fatigue syndrome" – with acronyms shortening it down to a manageable size: ME/CFS. This document was legally commissioned and approved by Health Canada. This is a legally enforceable document in relation to patient's rights. It can be enforced through a Canadian court. Many medical doctors now use the Canadian Consensus criteria (2003) to diagnose and treat patients in Canada. See documents below Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols, 2003
and For Medical Doctors - Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Diagnostic and Treatment Protocols, 2003 for doctors and specialists in Canada.
The Australian government also recommends use of the Canadia Consensus criteria (2003). This is outlined in the following Australian government web site http://sacfs.asn.au/download/guidelines.pdf
In Japan the Japanese Ministry of Health commissioned and approved a new definition in 2004 called 'Childhood Chronic Fatigue Syndrome', this detailed several immunological, neurological, sleep disorders,. endocrine, infectious factors in the illness. Childhood chronic fatigue syndrome. Miike T. Nihon Rinsho. 2007 Jun;65(6):1099-104.
In 2008, the Japanese Association of Fatigue Science which works closely with the Japanese Ministry of Health, published its definition, and diagnostic and treatment criteria for ME / CFS. Leading Japanese researchers and doctors were involved in this. It's defintion included immune system, neurological, endocrine and infectious factors. It was similar to the Canadian Consensus criteria (2003) and the later International Consensus criteria (2011). Though, the Japanese definition goes into a bit more detail. The Japanese Ministry of Health funds scientific research into the factors defined by the Japanese Association of Fatigue Science in their definition. Their defintion is being used in Japan at present. See papers below: Chronic Fatigue Syndrome Hirohiko Kuratsune,
Yasuyoshi Watanabe.
Fatigue Science for Human Health
2008, pp 67-88
Position paper - http://www.med.or.jp/english/pdf/2006_01/019_026.pdf
In Japan there is also a condition called called "Low natural killer cell syndrome" which is very similar to ME and CFS. Natural killer cell abnormalities are one of the most consistent findings in ME. The following papers outline the Japanese position on the illness. They correlate to some points in the aforementioned diagnostic criteria used by the Canadian and Norwegian governments.
- Aoki T, Usada Y, Miyakoshi H: A novel immunodeficiency: Low NK syndrome (LNKS). Jap J Med 3212:14-17, 1985
- Aoki T, Usuda Y, Miyakashi H, et al: Low natural syndrome: clinical and immunologic features. Nat Immun Cell Growth Regul 6:116-128, 1987
- Aoki T, Miyakoshi H, and Usada Y et al: Low NK syndrome and its relationship to chronic fatigue syndrome. Clin Immunol Immunopathol. 69:253-65, 1993.
The clinical features of low natural cell numbers, function and cytotoxicity is specific to ME and CFS and "Low natural killer cell syndrome"
The diagnostic criteria used by the Canadian, Australian and Norwegian governments and health authorities represent best international practises and the latest medical and scientific research findings. They also integrate the 'Low natural killer cell syndrome' findings used by the Japanese government into their criteria.
The scientific and medical evidence show that ME is a highly complex physical illness, involving multiple factors, encompassing immune system, endocrine system, mitochondria, brain and nervous system dysfunctions and abnormalities, and this is accompanied in most cases by chronic viral and / or pathogen infections at some stage of the illness.
5. The Harmful Effects of CBT and GET in ME / CFS cases. The Inefficacy of CBT and GET.
There have been many research findings and clinical findings which show the harmful effects of CBT and GET and exertion in ME / CFS patients. In addition to this, the inefficacy of CBT and GET in terms of lack of full recovery, lack of return to normal function, lack of normal health (prior to illness), lack of return to sporting and other social activities, lack of return to full time employment or full time education or training has also been shown. This research is listed in the links below
6. Preparing Legal casesfor Patients The best way for ME & CFS patients to win court cases is through:
get a good lawyer and / or barrister with experience in disability law and rights and in RICO charges and fraud charges against businesses / individuals.
get your lawyer / barrister to fully understand the illness, the biological evidence and the legal issues around it. Reading this web site may assist in this www.me-ireland.com and www.me-ireland.com/bogus.htm
gather and present a large amount of personal medical and scientific data on the illness, including the results of many tests. And making it easy for lay people and legal professionals to understand in court.
back this up with the results of scientific research papers.
back this up with biological based case definitions and diagnostic criteria of the illness to corroborate the above results and findings
corroborating this with patient testimony backed up by GP testimonies and medical specialist testimonies (attendance in court or by live video conference)
Back this up with live testimonies or sworn affidavitts from national & international medical experts and from leading scientists in court (attendance in court or by live video conference.
corroborating this with medical doctors who run biological based ME and CFS clinics and have had successes treating ME and CFS patients (attendance in court or by live video conference)
corroborating this with evidence of the damage done by GET and the ineffectiveness of CBT, including the testimonies of medical doctors, scientists and medical experts.
corroborating this with representatives from government funded bodies and national health authorities who have been well briefed on the illness (attendance in court or by live video conference)
backing this up with case laws and legal precedents from similar legal cases in the past
backing this up with passages from national laws, Constitutional provisions and human rights laws.
This is the level of detail and commitment required to win court cases.
7. Further Legal Analysis
Exposing Bogus Treatments based on Quackery, Corruption and Deception in ME / CFS
Quackery and alleged diagnosis based on presumptions, guesses, superficial judgments and assumptions with no scientific and medical basis, no patient examination and tests, and in many cases involving denigration, blaming and insulting of the patient still exists in the 21st century. There is a minority of psychiatrists and a minority of medical doctors with psychiatric leanings who wrongly believe ME / CFS to be a psychiatric illness and they interpret patient cases to suit their own preconceived notions and ideas, and thus they mislabel and misdiagnose patients. There have been many well publicised cases of doctors misdiagnosing patients as having mental illness, when they had Cancer, heart disease, artery and vein blockages, diabetes, Anti-NMDA receptor encephalitis, Behçet's disease, ME / CFS, Chronic lyme disease, Common Variable Immune Deficiency (CVID), Ehlers–Danlos syndrome (EDS), Neurological illnesses, mitochondrial disorders, serious Endocrine disorders, TB, MS and Sjögren's syndrome. They even ignored up to date diagnostic and treatment protocols using best international practises, and scientific and clinical findings, when seeing patients. Thus they disregard the very basis of medicine. Despite advances in technology and in particular sophisticated medical diagnostic technologies used in leading hospitals and medical clinics, this small minority of medical professionals continues to ignore them and refuses to use them. The end result is that sick patients were and still are deprived of an accurate diagnosis and proper treatments, and remain ill for years and decades.
A small minority of these medical professionals and researchers go further and actively manipulate or even create and recreate ambiguous entry criteria in scientific trials to suit their own needs, and then manipluate the trial itself and the results to fit in with their preconceived notions and views. From this they create false new syndromes, new paradigms and entities, and new "treatments" in medicine with no basis in medical and scientific fact and evidence. In fact, in many cases the biological evidence is ignored and deliberately not investigated so as to increase the chances of discovering a new somatic syndrome or somatoform disorder or psychiatric illness. This new syndrome is then cynically used as a money making machine.
The following news items present a well-known example of psychiatrists abusing their powers to call an illness "psychiatric" when in fact it was not a psychiatric illness, it was a physical, organic and biological illness. Some psychiatrists illegally imprisoned a young girl, Justina Pelletier in an inpatient mental health ward in Boston Children’s hospital in Massachusetts in 2013 and refused to accept the medical reports from doctors at Tufts University hospital and other medical doctors. This was carried out with the cooperation of The Department of Children and Families (DCF) who legally enforced this incarceration of Justina Pelletier. Her case consumed vast amounts of energy within a state agency already plagued in 2013/14 by child deaths under its watch, which led to the resignation of its Commissioner. She was incarcerated in the psychiatric ward against her wishes, against her family's wishes and against her doctors wishes, and against the wishes of doctors at Tufts University Hospital. The psychiatrists used a newly invented term "Somatoform Disorder" to imprison her in a psychiatric ward. While she was incarcerated, the psychiatrists refused to accept a second opinion from doctors, and deprived the child of her treatments for her physical, biological illness, thus depriving her of her legal and human rights. Her parents were only allowed to see her once a week, for one hour. She deteriorated while being imprisoned in the psychiatric ward, as her physical illness was completely neglected. It took a number of court cases in the USA and several public protests to get her released from this psychiatric unit and back to her family. She is now receiving treatment for her physical, biological illness. Her family will be taking legal actions against the DCF, the psychiatrists and the hospital involved. And legislators are considering changes to laws to stop this abuse permanently.
The illness ME / CFS has been a victim of this dishonesty and deception for many years. This has caused great division, social tensions and resentment and much unnecessary suffering and deaths worldwide. Yet none of this would have occurred if medical doctors, medical councils and associations, medical research councils, researchers, Universities, civil servants and politicians had stuck to the medical and scientific facts, first established by the Dr. Acheson in 1956 and later by the CDC and Dr. Cheney, Dr. Peterson and Dr. Holmes in the late 1980's, stating that ME / CFS was a biological, physical illness, not a psychiatric illness. There are now 5,000 scientific research papers proving that ME / CFS is a biological, physical illness, yet some disreputable individuals still falsely claim it is a psychiatric illness.
The Bigger Picture
Dr. Marcia Angell of the Harvard Medical School and former editor of the New England Journal of Medicine wrote a book called 'The Truth About the Drug Companies: How They Deceive Us and What to Do About It' and a famous article in the New York Review of Books called 'Drug Companies & Doctors: A Story of Corruption' and in these works she has stated that a lot of scientific research and some medical guidelines and drugs lack objective evidence, proof, efficacy, safety, integrity and credibility. The following quotes clearly express her dissatisfaction with this state of affairs
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”
“Thanks largely to him (Dr. Joseph L. Biederman), children as young as two years old are now being diagnosed with bipolar disorder and treated with a cocktail of powerful drugs, many of which were not approved by the Food and Drug Administration (FDA) for that purpose, and none of which were approved for children below ten years of age.”
Dr. Richard Horton, Editor-in-chief of the Lancet recently published a statement declaring that a shocking amount of published research is unreliable at best, if not completely false, as in, fraudulent. A shocking admission by the editor of the world's most respected medical journal, The Lancet, has been virtually ignored by the mainstream media. For more details read here Medical insider: "science has taken a turn towards darkness"
The role of some big pharma companies and insurance companies in paying certain psychiatrists, doctors and researchers through commissions, speaking fees at conferences, seminars, and meetings, lecture fees, consulting fees, writing fees, awarding of executive positions, holidays abroad or "travel expenses", share and stock options, bulk ordering of their books, benefits in kind, etc. is discussed and analysed. Some psychiatrists are actively encouraged to invent new illnesses and syndromes and even mislabel physical illnesses as psychiatric in order to create new markets for drugs. This has been reflected in dishonesty and manipulation of research trials. Her views are shared by many leading scientists and medical doctors. There has been a worrying trend in scientific research since the early 1990's, involving a departure away from scientific honesty, truth and integrity towards dishonesty, falsification, manipulation and deception for the acquisition of desired research results, profit, wealth, fame, prestigious awards, self-aggrandisement, career advancement and higher social status. The following research paper by Dr. John Ioannidas and others outlines the problems with scientific research in recent years.
Clinics to treat ME - 2 Different and Opposing Models There are vast differences between (a) clinics specialising in biological based immune system, anti-viral / anti-pathogen, neurological and endocrine treatments for ME (See listing of these Diagnosis and Treatment section) (b) clinics specialising in psychiatric diagnosis and treatments for ME. The psychiatric clinics have proven to be complete failures and a waste of taxpayers money and insurance companies' money, while clinics using biological based immune system, anti-viral / anti-pathogen, neurological and endocrine treatments for ME have proven to successful and have brought about significant improvements and recoveries. Proper medical and biological based ME clinics look at the biological facts and evidence through the use of proper diagnostic procedures (International Consensus criteria 2011, Canadian criteria 2003, Nightingale criteria 2007, known bio-markers, objective data, intensive biological testing, history and clinical symptoms) and identify ME, the number of abnormalities and dyfunctions present in the patient, the subgroup the patient belongs to, and the phase of the illness. From these facts and evidence, treatments are devised. These treatments are assessed regularly to measure their efficacy, and amended if necessary. Further testing after several months or a year, enables doctors to determine if progress is being made or not, and if full recovery is underway. The probability of full recovery increases as each biological abnormality and dysfunction is resolved over time. If the ME patients mentioned below had attended one of these clinics, they would have been diagnosed inside 6 weeks, and a full listing of the biological abnormalities and dysfunctions would be available to the doctors. They would then start treatment, and this would closely monitored over time. Their chances of full recovery would be high. They would still be alive today.
Psychiatric based clinics cannot diagnose or treat ME. These clinics provide psychiatric diagnosis based on filling out a few forms and questionnaires. The subjective opinions and views of a psychiatrist are also used in the diagnosis formation. Biological tests are not undertaken and are strongly discouraged by psychiatrists. They ignore serious immune system abnormalities, virus infections and other pathogen infections, HPA axis dysfunction, neurological dysfunctions, brain lesions, chronic allergy activation, methylation dysfunction, mitochondria and krebs cycle dysfunction, etc. They are presumed to not exist. These clinics are against testing patients as biological tests may undermine psychiatric presumptions. The pyschiatrist provides a psychiatric treatment, which involves CBT, GET and some psychiatric drugs which makes the patient even more tired. The side effects of these drugs are serious, and often involve tiredness, dry mouth, dizziness, confusion, diffiiculty concentrating, weakness, pain, headaches, etc. and this is even worse for ME patients as their liver function is impaired and they have problems detoxifying these drugs. GET or exercise therapy tends to worsen symptoms in most ME patients due to dysfunctions in the mitochondria, the krebs cycle, methylation cycle, anitoxidant systems, the muscular system, and the circulatory and vascular systems. This has been confirmed by scientific research. Though these facts are conventinatly ignored by the psychiatrists who run these clinics. The patient either remains sick or worsens over time. As time progresses, the psychiatrist informs the patient that he / she is improving gradually and making progress, when in fact they are not. No biological markers and objective data is used by psychiatrists to support their claims. Based on the presumption of the psychiatrist that progress is being made, the psychiatrist then makes a report on this, and then includes this in research papers submitted to medical journals. This then misinforms science and medicine, and creates a myriad of problems. The whole psychiatric diagnosis and treamtent of ME is based on presumptions, assumptions, suppositions and guess-work, and has no basis in biological facts and medical and scientific evidence. Psychiatrists should move out of the field of ME which is a physical, biological and organic illness, and move back into treating mental illnesses such as depression, bi-polar, schizophrenia, etc.
The NICE clinics in Britain are using treatments for psychiatric illnesses to treat ME, which is wrong, misguided and is not succeeding. Treatments such as CBT, GET and psychiatric drugs cannot bring about recovery from ME and are a waste of British taxpayers money. There have been no reports of full recoveries of ME patients in such psychiatric
clinics (NICE clinics). In fact there are many reports of ME patients
remaining ill or becoming worse after visits to such clinics. This is due to the fact
that ME involves several biological abnormalities and dysfunctions and chronic infections, and these cannot be effectively treated with psychiatric treatments. The following testimony by Professor Malcolm Hooper to the British House of Commons in 2007 shows the failure of NICE clinics in Britain - Evidence submitted by Professor Malcolm Hooper .
The NICE "CFS/ME" Guideline Development group excluded from its membership all NHS medical specialists and all medical doctors (GP's) experienced in treating ME patients. It was dominated by psychiatrists, psychologists and doctors with no experience of ME. Three of these had conflicts of interest involving insurance companies. A senior parliamentarians' inquiry group on ME in 2006:
"There have been numerous cases where advisers to the DWP [Department of Work and Pensions] have also had consultancy roles in medical insurance companies. Particularly the Company UNUM Provident. Given the vested interest private medical insurance companies have in ensuring CFS/ME remains classified as a psychosocial illness there is blatant conflict of interest here. The Group find this to be an area for serious concern and recommends a full investigation of this possibility by the appropriate standards body." Source: Parliam entary Group on the Scientific Research into ME (GSRME) Report, Page 30, November 2006: http://www.erythos.com/gibsonenquiry/index.html
These facts are shocking by any standards. Other factors worked to make the NICE guidelines biased, defective, misleading, ineffective, contradictory and erroneous, please read http://www.meactionuk.org.uk/The-UK-Governments-three-pronged-strategy-for-CFSME.htm .
There was a total disregard for the medical and scientific facts. Furthermore, the NICE guidelines advised against biological diagnostic tests for patients. Thus patients are deprived of diagnostics to identify the biological abnormalities, dysfunctions and infections which afflict them. The sad fact is that many British ME patients are suffering pain, hardship, and dying
of ME because the British government is being poorly advised by psychiatrists and as a result does not have proper ME
clinics to treat them. The following video shows a British woman who had ME and was given a bogus psychiatric diagnosis and psychiatric treatments by British doctors. These psychiatric treatments included CBT and exercise therapy. She died. A post-mortem revealed that she had a virus infection of the spinal cord and nervous system and a lot of inflammation of the spinal cord. Psychiatric treatments could not treat this, but some British doctors insisted on psychiatric treatment which led to her death. Click on videos below to watch them.
The Hippocratic oath taken by medical doctors states that a doctor should do no harm. Improper diagnosis and treatments and neglect of this woman through the wrong use of psychiatric medicine meant that serious harm was done to this woman. And, unfortunately many other ME patients are suffering similarly. In 2013 in Denmark, Karina Hansen, a child diagnosed with ME by a few medical doctors, was forcibly removed from her family home by police and psychiatrists and falsely imprisoned in a psychiatric clinic, against her own will and against the will of her parents and medical doctor. The psychiatrists ignored the diagnosis of medical doctors, and refused to offer diagnostics, laboratory tests, and medical treatments for ME. She was forced to take psychiatric drugs and her condition deteriorated. The psychiatrists blocked local Danish medical doctors and foreign medical doctors from seeing her. Thus, she was deprived of medical treatment for ME. As of 2014, her psychiatric treatment continues to be ineffective, and she is being kept against her will and against the will of her family and her family doctor. Her parents were blocked from visiting her. She received no treatment for ME. This is a disgraceful abuse of her human rights and has led to protests in Denmark and several other countries. Click on the follwing link to view letter addressed by Karina Hansen's parents to members of the Danish Parliament
The following news programme and documentary discusses this issue further.
There was another case of an ME patient in England who had serious enteroviral infection of the brain and nervous system and he was told by doctors that he was suffering from depression. He was given psychiatric drugs which made him worse. This neglect by doctors made him very ill and he deteriorated rapidly. He committed suicide. An autopsy revealed that he had serious enterovirus infection of the brain and nervous system. Read article here - https://listserv.nodak.edu/cgi-bin/wa.exe?A2=ind0112a&L=co-cure&F=&S=&P=62
One well known British psychiatrist (based in London) wrongly diagnosed a British woman with a psychiatric illness, when she actually had a physical illness known as Ehlers–Danlos syndrome (EDS). The psychiatrist did not bother to carry biological-based diagnostic tests on the woman, but he made his own diagnosis via presumptions and assumptions and added insult to injury by accusing her of having no illness and that it was "all in the mind". (Article by Ehlers–Danlos syndrome patient). There was a case of a woman who had ME/CFS and she was wrongly diagnosed with a psychiatric disorder by psychiatrists. Intensive biological tests revealed mycoplasma infection which caused intestinal abnormalities, inflammation, immune dysfunctions, sleep disorder and extreme exhaustion. After treatment with antiobiotics and rest, she recovered ( Maes M, Coucke F, Leunis JC: Normalization of the increased translocation of endotoxin from Gram negative enterobacteria (leaky gut) is accompanied by a remission of chronic fatigue syndrome. Neuro Endocrinol Lett 2007, 28:739-744.). Psychiatrists were proven wrong in this case and in many cases involving ME and other physical illnesses.
Another similar case in the USA occurred where a woman was admitted to a New York hospital. She had neurological dysfunctions resulting from viral infection of the brain and nervous system and immune-related inflammation of the brain. The psychiatrists presumed that she had a psychiatric illness and they took charge over her. They gave her psychiatric drugs which did not work. She was eventually referred to a virologist. After some tests, the virologist diagnosed Anti-NMDA receptor encephalitis. The woman received medical treatment for this, and she gradually recovered over the course of one year. ( 'Brain on Fire' by Susannah Cahalan, Free Press, 2012. And Mail Online article.)
There are many cases of psychiatrists wrongly diagnosing people with psychiatric illness, when in fact they had physical illnesses, such as chronic viral or pathogens infections, immune system dysfunctions, neurological illnesses and autoimmune diseases which caused injury to the brain and nervous systems. This failure of psychiatry is serious, in the sense that it puts lives in danger, and it is time for medicine to make a clear distinction between psychiatric illnesses which are diagnosed with precision via biological tests and psychological tests and physical illnesses which are diagnosed with precision via biological tests.
Why ?
Most of the medical and scientific community worldwide now accepts that ME is an organic, physical illness involving dysfunctions in the immune system, and nervous system, HPA axis and endocrine systems, and infections at some stage of the illness. This is backed up by 5,000 scientific research papers proving this is a biological and biomedical illness. The evidence of this is beyond reasonable doubt. This is now accepted by governments and health departments around the world. The CDC and the NIH in the USA which are the top medical and scientific research institutes in the world also accept this. Yet all of this is ignored and denied by certain British psychiatrists who wrongly claim it is a psychiatric illness. In Britain these particular psychiatrists have hijacked ME diagnois and treatment and made it into a psychiatric illness when it is not. They have manipulated politicians and civil servants to support their psychiatric agenda, and control ME treatment within the NICE clinics. Hundreds of thousands of people are being denied proper medical treatment for a physical illness and being given bogus psychiatric treatment, and they remain sick and cannot recover as a result.
These particular psychiatrists have also ignored the medical and clinical findings from medical clinics and hospitals around the world which show that certain medical treatments based on biological and biomedical evidence can lead to recovery in many cases (1). And a significant improvement in the condition in all cases (1). It is un-scientific and unethical for these psychiatrists to ignore all of this and the overwhelming biomedical research findings from around the world. These few psychiatrists are seen as misfits by much of the medical and scientific community around the world.
Research into the reasons behind the actions of these few psychiatrists reveal the following:
(a) there has been an intense "turf war" between medical doctors and psychiatrists over physical illnesses such as ME, fibromyalgia, Gulf war illness, irritable bowel syndrome, chronic pelvic pain, chronic organophosphate poisoning, and other illnesses which are not fully understood by science, but biological and biomedical research suggests that they are biological illnesses which are complex and multi-faceted. These illnesses are worth many millions of euros to whichever side takes control over them - either the medical doctors or the psychiatrists.
In 1970 two psychiatrists McEvedy and Beard published a paper claiming that M.E. was a psychiatric disorder and that it was "all in the mind". The authors of this paper did not physically examine the patients, did not interview the patients, did not consult with the medical doctors and medical records of the patients. They merely superficially reviewed a few studies. The paper was a fraud, and was not based on a clinical examination of patients and biological and biomedical evidence and the biological testing and interview of patients. The paper was based on the presumptions and assumptions of two psychiatrists who knew nothing about the illness. The paper provoked a furious backlash from medical doctors and nurses who fell ill with M.E. Doctors, nurses and patients wrote letters in to the British prress and to medical and scientific journals rejecting the hypothesis of McEvedy and Beard. In 1978, The Royal Society of Medicine rejected the paper of McEvedy and Beard and their presumptions and stated that ME was a physical, biological illness involving infection and neurological, immune system and endocrine abnormalities - British Medical Journal, June 1978. This settled the matter in Britain and remained the position of the British Medical authorities and British government until the early 1990's. Dr. Byron Hyde a famous Canadian medical doctor wrote an interesting account of this in the following booklet - A Brief History of Myalgic Encephalomyelitis.
Then in 1991 and the early 1990's, a few psychiatrists managed to hijack the term ME (CFS) and falsely claimed it to be psychiatric illness and "all in the mind". Over several years, they used their influence over government ministers, government departments, the press and media centres, the Medical Research Council, the Medical Council, the Royal Society of Medicine, the NHS, and government sponsored committees to convince them that ME (CFS) was psychiatric, "all in the mind", a non illness. In addition, scientific papers about the biological aspects of ME (CFS), encompassing immune system, neurological, endocrine abnormalities and infections, were blocked and not published by reputable medical journals in Britain, but were published in the USA, Canada, the EU and other countries. Furthermore, scientific research into the biological causes and perpetuating factors in ME (CFS) was blocked by a small group of psychistrists "advising" and working within the Medical Research Council, over a period of twelve years. While psychiatric research into ME (CFS) was fully funded by the Medical Research Council.
Secret Files
This has been confirmed via disclosure of some of the secret files hidden away until 2071 at the UK National Archives at Kew in Britain. Mrs. Valerie Smith posted these on her blog a few years ago. These are important historical documents detailing (i) the denial of scientific and medical facts by certain psychiatrists (ii) the lies and disinformation of certain psychiatrists (iii) the manipulation and subversion of state bodies. It provides shocking and disturbing facts (which can be used in court cases).
- national-archives.pdf
- national-archives1.pdf
Dr. Melvin Ramsey who first defined M.E. in the 1950's and spent 40 years treating ME patients and researching the illness had the folowing criticisms of psychiatry
' Routine physical examination and the ordinary run of laboratory investigations usually prove negative and the patient is then often referred for psychiatric opinion. In my experience this seldom proves helpful is often harmful; it is a fact that a few psychiatrists have referred the patient back with a note saying 'this patient's problem does not come within my field'. Nevertheless, by this time the unfortunate patient has acquired the label of 'neurosis' or 'personality disorder' and may be regarded by both doctor and relatives as a chronic nuisance. We have records of three patients in whom the disbelief of their doctors and relatives led to suicide; one of these was a young man of 22 years of age.
The too facile assumption that such an entity - despite a long series of cases extending over several decades - can be attributed to psychological stress is simply untenable. Although the aetiological factor or factors have yet to be established, there are good grounds for postulating that persistent virus infection could be responsible. '
Dr. Melvin Ramsey had further criticisms of exercise and psychiatry
' in those patients whose dynamic or conscientious temperaments urge them to continue effort despite profound malaise or in those who, on the false assumption of 'neurosis', have been exhorted to 'snap out of it' and 'take plenty of excercise' the condition finally results in a state of constant exhaustion. This has been amply borne out by a series of painstaking and meticulous studies carried out by a consultant in physical medicine, himself an ME sufferer for 25 years. These show clearly that recovery of muscle power after exertion is unduly prolonged. After moderate excercise, from which a normal person would recover with nothing more than a good night's rest, an ME patient will require at least 2 to 3 days while after more strenuous excercise the period can be prolonged to 2 or 3 weeks or more. Moreover, if during this recovery phase, there is a further expenditure of energy the effect is cumulative and this is responsible for the unrelieved sense of exhaustion and depression which characterises the chronic case. The greatest degree of muscle weakness is likely to be found in those muscles which are most in use; thus in right- handed persons the muscles of the left hand and arm are found to be stronger than those on the right. Muscle weakness is almost certainly responsible for the delay in accommodation which gives rise to blurred vision and for the characteristic feature of all chronic cases, namely a proneness to drop articles altogether with clumsiness in performing quite simple manoeuvres; the constant dribbling of saliva which is also a feature of chronic cases is due to weakness of the masseter muscles. In some cases, the myalgic element is obvious but in others a careful palpitation of all muscles will often reveal unsuspected minute foci of acute tenderness; these are to be found particularly in the trapezii, gastrocnemii and abdominal rectii muscles.'
Yet even in 2013, despite all the biological and biomedical evidence accumulated that it is a physical, biological illness, some psychiatrists still choose to believe the falsehoods of McEvedy and Beard in 1970 (7).
(b) Rejection of Science. Some psychiatrists have attempted to convert physical and biological illnesses into psychiatric illnesses for their own financial gain and for the attainment of status, awards and prestige. And in the process, they have ignored and dismissed biological and biomedical evidence, some 5,000 research papers. Psychiatry has not produced any biological evidence that ME is a psychiatric illness. This failing by psychiatry and the intense efforts of psychiatrists to dismiss and reject biological findings and biomedical research represents a rejection of science, the scientific method and causality, and the scientific ideals which emerged from the Age of Enlightenment.
The statement of Dr. Byron Hyde, a Canadian medical doctor who has treated thousands of ME patients since 1985 sums up the attitude of many medical doctors who treat ME patients
' M.E. is not depression; M.E. is not hysteria; M.E. is not a conversion disorder nor is it a somatization disorder; M.E. is an acute onset diffuse
injury of the brain. Psychiatrists should not ever be
placed in charge of diagnosis and treatment of M.E.
patients. It is simply not their area of expertise and
their meddling has at times caused great harm to M.E.
patients. Also, during the 20 years that I have
investigated M.E. patients I have yet to see a single
case of real M.E. that has responded to psychiatric
pharmacological treatment such that the patient has
recovered and been able to return to work or school. ' The Nightingale Definition of Myalgic Encephalomyelitis (M.E.) Dr. Byron Hyde
This is supported by Dr. Anthony Komaroff, Professor of Medicine at Harvard Medical School in the USA. He has been treating ME patients and researching the illness since 1987. He has stated the following:
' many patients with ME / CFS have no diagnosable psychiatric disorder and that ME / CFS is not a form of depression; ' Source: Summer 2008 issue of The CFIDS Chronicle published by The CFIDS Association of America.
Video Lectures on ME, FM and Gulf War Illness and other Neurological illnesses by scientist and Sunderland University Professor, Dr. Malcom Hooper. Videos 1 - 10
(c) Psychiatrists are in conflict with other psychiatrists over the concept of 'somatic syndrome' and the fact that some psychiatrists are trying to allege physical, biological illnesses are psychiatric, when they are not. The ignoring of medical and biological evidence by psychiatrists is also a major point of debate. The following clinical evidence and scientific papers and works below present this problem in some detail :
The work of psychiatrists - Dr. Thomas Henderson and Dr. William Pridgen
Valacyclovir treatment of chronic fatigue in adolescents. Henderson TA. Adv Mind Body Med. 2014 Winter;28(1):4-14.
(d) In 1988, the CDC created a defintion for CFS, this is often called the Holmes definition after Dr. Gary Holmes, a well known CDC researcher. This defintion specifically excluded psychiatric illnesses :
" Other clinical conditions that may produce similar symptoms must be excluded by thorough evaluation, based on history, physical examination, and appropriate laboratory findings. These conditions include.......................................................chronic psychiatric disease, either newly diagnosed or by history (such as endogenous depression; hysterical personality disorder; anxiety neurosis; schizophrenia; or chronic use of major tranquilizers, lithium, or antidepressive medications);............................................" CDC Definition of CFS, 1988
This was created by the CDC in order to establish CFS as a physical and biological illness, not a psychiatric illness. This has been conveniently ignored by some psychiatrists and a minority medical doctors since 1988.
The 1994 CDC criteria specifies the following exclude a diagnosis of Chronic Fatigue Syndrome
"Any past or current diagnosis of:
major depressive disorder with psychotic or melancholic features
bipolar affective disorders
schizophrenia of any subtype
delusional disorders of any subtype
dementias of any subtype
anorexia nervosa
or bulimia nervosa
This also was created by the CDC in order to establish CFS as a physical and biological illness, not a psychiatric illness. And again, this has been conveniently ignored by some psychiatrists and a minority medical doctors since 1994.
(e) How odd it was that the Wessely school psychiatrists managed to omit the psychiatric exclusion in the Holmes CDC criteria from their own Oxford definition. Yet the Oxford defintion was supposedly based on the Holmes CDC criteria.
The 1988 Holmes CDC Definition
" Other clinical conditions that may produce similar symptoms must be excluded by thorough evaluation, based on history, physical examination, and appropriate laboratory findings. These conditions include.......................................................chronic psychiatric disease, either newly diagnosed or by history (such as endogenous depression; hysterical personality disorder; anxiety neurosis; schizophrenia; or chronic use of major tranquilizers, lithium, or antidepressive medications);............................................" CDC Definition of CFS, 1988
This contradiction between the Holmes CDC criteria and Wessely school's Oxford defintion undermines the validity of the Oxford definition.
(f) CDC in USA
"CFIDS has an organic basis; it is
not
a psychiatric illness. Our Surveillance Study does not
support the notion that (ME)CFS is a psychiatric illness, and in fact, suggests that it has an
organic basis"
Dr Walter Gunn, Principal Investigator of (ME)CFS studies at the US Centres for
Disease Control: CFIDS Chronicle, February 1992, page 1
In 2013, the CDC (USA) published the results of a CDC multi-clinic study into ME/CFS. They found several physical & biological abnormalities in patients. They also reported that the vast majority of ME/CFS patients had normal mental health, and they coped well with a debilitating physical illness. This repudiates the opinions and views of Wessely school psychistrists.
Read: http://www.cortjohnson.org/blog/2013/05/11/first-fruits-of-cdc-chronic-fatigue-syndromemulti-clinic-study/
(g) some psychiatrists have conflicts of interest, that being very close links to health insurance companies. Some of these psychiatrists have acted as advisors, consultants and have been given executive positions in insurance companies. These companies have made massive savings from the denial of proper biological diagnostics and treatments for ME patients (2). This denial of necessary medical treatment has kept many patients ill for years and decades and contributed to deaths from the illness. Psychiatrists have made money from commissions, speaking fees at conferences, seminars, and meetings, lecture fees, consulting fees, writing fees, awarding of executive positions, holidays abroad or "travel expenses", share and stock options, bulk ordering of their books, benefits in kind, etc..
For several years, some psychiatrists prevented government research bodies from funding and investigating the biological causes of the ME and CFS, so that they could promote psychiatric based explanations and treatments. This also enriched certain insurance companies. Psychiatric treatments such as cognitive behaviour therapy and graded exercise therapy and psychiatric drugs are far cheaper and far inferior than other treatments such as anti-viral, anti-pathogen and immune system, endocrine, mitochondria and neurological treatments. Instead of investing in people's health and full recovery, they are investing in cheap, inferior and ineffective treatments which impose higher costs on everybody and society in the medium to long term. (2,7).
For further clarification on conflicts of interest, read the following papers and watch the following news videos
Videos about Insurance companies which denied disabled people their lawful payments. Some of these have advised governments. Some psychiatrists work as consultants, advisors, or executives for these insurance companies.
(h) some psychiatrists have claimed that they are saving the government money by classifying it as a psychiatric illness and forcing patients to undergo, cheap, inferior and ineffective psychiatric treatments which keep them ill. Yet these bogus psychiatric treatments impose huge costs on the economy, the government and society, through losses in productivity, in GNP and taxes which would have been earned by these patients if they had been given the proper medical treatment and recovered.
Ireland: 1.83 billion euros per year Britain: £20 billion per year USA: $90 billion per year
One example of this is the 'Occupational Aspects of the Management of
Chronic Fatigue Syndrome: a National Guideline', DH Publication 2006/273539 in Britain which as failed many ME and CFS patients there. A report which includes conflicts of interest. These are enormous losses to economies. Why should some psychiatrists be allowed to enrich themselves from ineffective, usless treatments with no scientific basis ? There are also conflicts of interest in relation to psychiatrists and government departments in some countries, for example the British Department of Work and Pensions, see www.meactionuk.org.uk/Obs_on_DLA_ Handbook_for_Gibson.html.
(i) Psychiatrists have helped big drug companies make more money from prescribing psychiatric drugs for ME patients. These psychiatrists were paid through commissions, speaking fees at conferences, seminars, and meetings, lecture fees, consulting fees, writing fees, awarding of executive positions, holidays abroad or "travel expenses", share and stock options, bulk ordering of their books, benefits in kind, etc. The more patients they can label as "psychiatric", the more money the psychiatrists can make. The DSM used by psychiatrists has been discredited by doctors, psychiatrists and psychologists. The following video presents these facts:
During the atomic bomb tests in the 1940's and 1950's
, the US Public Health Services were instructed to tell citizens downwind from bomb tests that the increases in cancers were due to neurosis, and that women with radiation sickness, hair loss, and burned skin were suffering from "housewife syndrome". (Goliszek, 2003: pp. 132–134). Psychiatrists were used to support these lies. This shows how psychiatry is used to cover up physcial and biological illnesses. It was an outrageous abuse of human rights at the time.
Over time some psychiatrists try to deny what they said in previous years so that they can continue manipulating a situation to their advantage. Its important to keep an account of what was said in the past and hold these people to account. Quotes from Wessely, Sharpe and White and others associated with them
(k) Evidence that the Wessely School psychiatrists know that CBT and GET provide no lasting benefit in ME/CFS
Despite their ruthless determination to implement CBT and GET across the board for people with ME/CFS, Wessely School members have previously acknowledged that there is no long-term benefit from CBT, for example:
at the American Association for CFS (AACFS, now the IACFS/ME) International Conference at Cambridge, Massachussets on 10-11th October 1998, Wessely School psychiatrist Michael Sharpe went on record stating that the benefits of CBT faded with time
in a personal communication dated 12th October 1998 to Professor Fred Friedberg, Michael Sharpe stated about his often-quoted 1996 study (BMJ 1996:312:22-26) that outcome measures had begun to decline 17 months after treatment termination (quoted in JCFS 1999:5:3/4:149-159)
on 3rd November 2000, Sharpe again confirmed: “There is a tendency for the difference between those receiving CBT and those receiving the comparison treatment to diminish with time due to a tendency to relapse in the former” ( www.cfs.inform/dk )
the very modest benefit in only some patients who have undergone CBT has been shown to last for only 6-8 months and “observed gains may be transient” (Long-term Outcome of Cognitive Behavioural Therapy Versus Relaxation Therapy for Chronic Fatigue Syndrome: A 5-Year Follow-Up Study. Alicia Deale, Trudie Chalder, Simon Wessely et al. Am J Psychiat 2001:158:2038-2042)
in his Summary of the 6th AACFS International Conference in 2003, Charles Lapp, Associate Clinical Professor, Duke University and Director, Hopkins-Hunter Centre, NC, stated about CBT that Dr Daniel Clauw (who had studied 1,092 patients) found that at 3 months there were modest gains, but at follow-up at 6 and 12 months, those modest gains were lost (this being an example of “evidence-based” medicine)
Wessely himself is on record stating that CBT doesn’t work for all: in his Editorial (JAMA 19th September 2001:286:11) he stated that CBT and GET are only “modestly effective” and that neither is “remotely curative”
Wessely is also on record as stating: “It should be kept in mind that evidence from randomised trials bears no guarantee for treatment success in routine practice. In fact, many CFS patients, in specialised treatment centres and the wider world, do not benefit from these interventions” (The act of diagnosis: pros and cons of labelling chronic fatigue syndrome. Marcus JH Huibers and Simon Wessely. Psychological Medicine 2006:36: (7): 895-900).
It should not be forgotten that after a course of CBT, there is no objective evidence of improvement (only subjective) and that the transient gains may be illusory (Interventions for the Treatment and Management of Chronic Fatigue Syndrome – A Systematic Review. Whiting P, Bagnall A-M et al. JAMA 2001:286:1360-1368).
Some psychiatrists have chosen to ignore this biological evidence as it conflicts with their viewpoints and opinions
(m) by converting ME into a psychiatric illness, psychiatrists can make a lot of money from patients and from the government (7). This has proven to be financially lucrative for many psychiatrists. And the fact that ME patients don't recover from the use of psychiatric treatments and this continues for many years and decades, means the psychiatrists can keep milking the system over time.
(n) Psychiatry is an inexact and imprecise science. It relies on subjective opinions and views not on medical and scientific facts and evidence. ME is not depression and not mental illness. The following article supported by research findings shows this
For example, Audrey Frost, an Irish woman suffered from a severe autoimmune and neurological illness which doctors failed to diagnose. The doctors did not carry out a full range of diagnostic tests, and they presumed that she had a psychiatric illness and sent her to a psychiatrist. She was then admitted to a psychiatric hospital, where her condition deteriorated. The psychiatrists refused to give her diagnostic tests to identify physical illness. They gave her psychiatric drugs, exercise therapy and CBT but these failed, and made her worse. Finally, her father demanded and paid for diagnostic tests for physical illness. She was diagnosed with Guillain-Barré syndrome an autoimmune and neurological illness. She received treatment and recovered gradually.
The psychiatrists were wrong and the psychiatric treatments were wrong and worsened the patient. Unfortunately, this is a regular occurance in many countries. Read news report below: http://www.independent.ie/life/health-wellbeing/it-started-with-a-simple-cold-and-ended-with-me-being-admitted-to-a-psychiatric-hospital-30444362.html
(o) Abuse, Harrassment and Insults of ME and CFS patients by some psychiatrists
The following document contains quotes from certain psychiatrists in relation to ME and CFS and patients. Some of it is deeply insulting, offensive and abusive of patients.
More examples of these insults and abuse of patients include the following:
' It is also a matter of record that in 2002, the BMJ ran a ballot asking doctors to vote on what they considered to
be "non-diseases" that are best left medically untreated and Wessely is believed to have proposed ME. Along
with freckles and big ears, ME was voted a "non-disease" and in April 2002 both broadsheet and tabloid
newspapers ran banner headlines proclaiming that ME is a non-disease. As a direct result, patients with ME/CFS
were removed from GPs' lists on the basis that "This practice does not treat non-diseases".
|
To dismiss a serious neuro-immune disease from which patients die as confirmed by UK Coroners' reports --
with such ridicule is shocking. '
Source:The Role of the Science Media Centre and the Insurance Industry in ME/CFS: the facts behind the fiction by Dr. Malcolm Hooper September 2013
Some psychistrists have recently invented a wide variety of new syndromes which they claim explains ME and CFS and Fibromyalgia and other illnesses. A few British psychiatrists recently created a new psychiatric term "general functional somatic syndrome" for certain illnesses such as irritable bowel syndrome (gastroenterology); chronic pelvic pain (gynaecology); fibromyalgia (rheumatology); non-cardiac chest pain (cardiology); tension headache (neurology); Gulf war illness; hyperventilation syndrome; and chronic fatigue syndrome (infectious disease). One psychiatrist in particular has in his "scientific " papers presumed that they are all alike and much the same; and he conveniently ignores the biological evidence which shows siginificant differences between them. He refuses to accept the biological and biomedical aspects of these illnesses and he refuses to deconstruct the biological and biomedical aspects of these illnesses into their constitutent parts and outline their biological dynamics, yet he makes broad sweeping generalisations about these illnesses. He totally ignores the clinical findings of leading medical doctors in the field. This is both un-scientific and unethical. It's another way of saying they are "all in the mind", not real physical illnesses. This is enabling psychiatrists to hijack these illnesses, label them all as psychiatric and cynically make money out of them (7).
Over time some psychiatrists try to deny what they said in previous years so that they can continue manipulating a situation to their advantage. Its important to keep an account of what was said in the past and hold these people to account. Quotes from Wessely, Sharpe and White and others associated with them
A Danish psychiatrist is using similar tactics to create an entirely new illness called "Bodily Distress Syndrome". He is lumping Fibromyalgia, Irritable Bowel Syndrome and Chronic Fatigue Syndrome together to form a new illness. Another recently invented illness or syndrome is "Bodily Stress Sydrome" and this merges some aspects of "Somatic Symptom Disorder" and "Bodily Distress Syndrome" and also lumps Fibromyalgia, Irritable Bowel Syndrome and Chronic Fatigue Syndrome together and claims they are forms of anxious depression. This "Bodily Stress Syndrome" is now competing with "General Functional Somatic Syndrome" and "Bodily Distress Syndrome" and "Somatoform Disorders" and other such nonsense to lump many separate illnesses together and call them one illness. In all cases, they ignore the biological evidence and biomedical research findings and the clinical findings of leading doctors in the field. Furthermore, these newly invented psychiatric syndromes contradict each other, and confuse the psychiatrists and everybody else, perhaps the psychiatrists suffered from over-imaginative minds (mental illness ?) and were too eager to create new syndromes. And they are actively manipulating politicians and civil servants and international bodies to believe these falsehoods and nonsense and make it official at national level and international level.
One well known British psychiatrist wrongly diagnosed a British woman with a psychiatric illness, when she actually had a physical illness known as Ehlers–Danlos syndrome (EDS). The psychiatrist did not bother to carry biological-based diagnostic tests on the woman, but he made his own diagnosis via presumptions and assumptions and added insult to injury by accusing her of having no illness and that it was "all in the mind". (Article by Ehlers–Danlos syndrome patient) Another similar case in the USA occurred where a woman was admitted to a New York hospital. She had neurological dysfunctions resulting from viral infection of the brain and nervous system and immune-related inflammation of the brain. The psychiatrists presumed that she had a psychiatric illness and they took charge over her. They gave her psychiatric drugs which did not work. She was eventually referred to a virologist. After some tests, the virologist diagnosed Anti-NMDA receptor encephalitis. The woman received medical treatment for this, and she gradually recovered over the course of one year. ( 'Brain on Fire' by Susannah Cahalan, Free Press, 2012. And Mail Online article.) New research recently released shows that many people diagnosed with mental illnesses had severe viral infections of the brain accompanied by inflammation-related injury and damage caused by over-active immune systems and / or autoimmunity. There are many cases of psychiatrists wrongly diagnosing people with psychiatric illness, when in fact they had physical illnesses, such as viral, immune system dysfunction and autoimmune illnesses which caused injury to the brain and nervous systems. This failure of psychiatry is serious, in the sense that it puts lives in danger, and it is time for medicine to make a clear distinction between psychiatric illnesses which are diagnosed with precision via biological tests and psychological tests AND physical illnesses which are diagnosed with precision via biological tests.
These same psychiatrists are attempting to label many physical illnesses as 'somatic syndromes' which is ridiculous, misguided, wrong, unethical and unscientific and goes against the scientific method and the medical method. The presumptions and assumptions inherent in their 'somatic syndrome' hypothesis, conveniently ignore the part played by chronic infections such as mycoplasmas, Lyme, Brucella, Chlamydia, viruses and other pathogens in the development of human illnesses, immune dysfunctions, neurological dysfunctions, mitochondria damage and dysfunctions, endocrine dysfunctions, organophosphate toxicity, household and work chemical toxicity, other biological and chemical exposures, and heavy metal toxicity. Research has revealed that there is an average of 140 toxic chemicals, heavy metals and pollutants in the human body. Research also shows that there are 200 toxic chemicals, heavy metals and pollutants in the umbilical cord of babies when they are born. Since 1945 there has been a massive increase in environmental toxins which has found it's way into human food, water, liquids, air and human bodies, and there has been an accompanying increase in toxin related illnesses such as Cancer, irritable bowel, Gulf War Syndrome and autoimmune diseases, including ME and Fibromyalgia (The Autoimmune Epidemic, Donna Jackson Nakazawa. Touchstone. 2009). It is known that toxins can damage mitochondria and interfere with the Krebs cycle, and cause changes and mutations to genes, neurological damage, and other multiple effects on the body. Many people have recovered from these illnesses after intensive detoxification combined with medical treatment for physical disease processes.
Gulf War Illness, like ME has been labelled a 'somatic syndrome' by these psychiatrists. Gulf War Illness shares many biological similarities with ME. In some cases people with Gulf War Illness were even diagnosed with ME. It has been established through scientific research in the USA that Gulf War Illness was caused by a combination of :
(i) exposure to depleted uranium in exploded shells
(ii) biological warfare agents which were released into the air through bombing of Iraqi chemical and biological weapons sites
(iii) pesticide exposures during the war
(iv) the effects of multiple vaccines on the immune system and body. Some soldiers had up to 20 vaccines given just prior to the war. Some vaccine batches were contaminated with mycoplasmas, bacteria and other pathogens.
(v)
exposure to viruses, parasites and bacterial infections.
(vi) fumes from burning oil wells
(vii)
adverse reactions to anti-nerve gas tablets
The first Gulf war was one of the most toxic wars in history. It was the first war where western soldiers were directly and indirectly subjected to multiple toxins and chemicals in a short period of time. These toxins and chemicals caused various biological dysfunctions and abnormalities and susceptibility to infections, genetic mutations and birth defects in offspring, and even Cancers in soldiers which lasted for many years after the gulf war. Much of this scientific and medical evidence was ignored. Yet psychiatrists were hired by the military and by governments to wrongly claim that it was a psychiatric illness and "all in the mind", a somatic syndrome. This misdiagnosis led to the deaths and severe suffering over many years of many ex-soldiers. Unfortunately this has occurred in other illnesses and diseases.
The following video lectures by Dr. Malcolm Hooper and Dr. Garth Nicolson sheds light on this
Video Lectures by Dr. Malcom Hooper. Videos 1 - 10
The scientific and medical communty need to further investigate the effects of these environmental toxins on the human body and establish standardised diagnostic standards and treatment protocols which could be mainstreamed in all medical practises, and dismiss the presumptions, 'somatic syndromes', assumptions, prejudices and hearsay of some psychiatrists.
(q) Research by Jason et. al. (4), and the findings of the Canadian definitions scientific researchers (5) clearly show that research projects based on CDC criteria and Oxford criteria and London Criteria often recruited patients who did not have ME but had other illnesses such as depression, mental illness, chronic fatigue, and other illnesses some un-diagnosed. Some psychiatrists have used the Oxford Criteria which is vague, inaccurate and ineffective in research trials into ME, and then recruited patients with mental illnesses, but wrongly classified them as having ME for their "scientific" trials (4,5,7). Furthermore, while selecting patients for trials, the psychiatrists conveniently ignored (4,5,7) and did not use the Canadian Criteria (3) which are based on biological and biomedical evidence. The biomarkers for the main physical abnormalities and dysfunctions and infections in ME were completely ignored in these trials, and this important ommission adds further evidence to the fact that many of the patients in these trials did not have ME (4,5,7) . Seriously ill patients who were bed bound or in wheelchairs were excluded from the trials, even though they were the most likely to actually have ME.
(r) Most psychiatrists see the world through the lens of psychiatry. They see and classify things in psychiatric terms. It's a state of mind. It is in their nature to view many physical illnesses as psychiatric and this is certainly the case when an illness is new. For example, psychiatrists once labelled MS and Parkinsons disease as mental illnesses and used psychiatric drugs to treat them. And if there are financial benefits or fame to be acquired from labelling a physical illness as psychiatric, then some will do this.
Some psychiatrists reject the PACE trial and the labelling of ME / CFS as psychological. Read the works of Dr. Thomas Henderson and Dr. William Pridgen
Valacyclovir treatment of chronic fatigue in adolescents. Henderson TA. Adv Mind Body Med. 2014 Winter;28(1):4-14.
(s) Social and cultural conditioning in some societies also means there is a reluctance to question authority and to challenge authority, and this has been exposed in the recent banking scandals, insurance scandals, political scandals, newspaper scandals, church scandals, show-business and television scandals, etc. in several countries. For example, the famous television star Jimmy Saville, had a knighthood from the Queen and a knighthood from the Pope, and was a respected and credible member of the British establishment, but he was a notorious pedaphile and had abused many people. He was only exposed after his death. All of these abuses by "respectable" and "credible" people proceeded from the fact that most people were afraid to question and to challenge corrupt authorities. Many ill people remain ill because good people of integrity refuse or are afraid to stand up and challenge corrupt authorities. This problem still exists.
(t) The devastating effect of psychiatry and stigma on ME patients and families
The success in explaining ME to anyone is dependent on their state of intelligence, their knowledge of the illness (which is almost zero in this country), their level of consciousness, the dominant messages and themes in the press, tv and media, and their ability to empathise with the suffering of another human being and willingness to accept people as they are regardless of disability or other perceived differences. We have to accept that many people, including well-meaning people, lack one or most of these factors, yet they would presume to be full of good intentions. The best thing they can do is learn about the illness, through reading www.me-ireland.com and other web sites, and learning to have empathy with a suffering humanity. Unfortunately the psychiatrists by wrongly calling ME a psychiatric illness which is "all in the mind" and "non illness" have caused great harm to ME patients and this has led to society and other people condemning, judging, criticising, and even physically attacking ME patients, and stigmatising them. Examples of this abuse of and mistreatment of ME patients include:
- being told " it's all in the head", "its all psychiatric", "its a
non illness", "too lazy to get out of bed", "too lazy to
work", "liar, you are able to work", etc. etc. ME patients in Ireland and
other countries have been subjected to insults, nasty abuse, gossip,
backbiting, criticism, judgmental attitudes, hateful and condascending comments. Being laughed at and mocked. This often leads to
conflict
- loss of friends who become insulting, critical and judgmental of the ME patient. Social
isolation of the ME patient.
- loss of contact with family members who become insulting, critical and
judgmental of the ME patient. Social isolation of the ME patient.
- being subject to violent physical attack by judgmental people and criminals. Often, ME patients end up in social or public housing
or bad private rented housing where there is many social problems and
criminality. ME patients are seen as easy targets.
- some doctors, consultants and nurses have insulted ME patients with abusive comments regarding the illness. This is
particularly bad as patients rely on doctors and nurses.
- break up of marriages and relationships. Most ME patients end up alone
as the social stigma of the illness destroys their ability to form
relationships. And the illness imposes limitations on the ME patient
functions in relation to forming and maintaining relationships.
- denial of health insurance payments by insurance companies and disability payments by government. Discrimination when seeking work.
- suffereing stigma and becoming the subject of gossip and nasty backbiting in the community.
- destitution from inability to work. The economic austerity and continued
cuts to disability payments and unemployment payments are a factor here.
All of these factors have a destructive effect on patients, and arise from the fact that some psychiatrists (a minority) have applied a wrong and misleading label on ME patients, and used their influence over government and the press and media to reinforce this label. This has had a devastating social effect on ill patients and their families.
(u) some psychiatrists were desperate to achieve fame and recognition as soon as possible and they thought they could do this by hijacking ME and converting it into a psychiatric illness. They then proceeded to write "scientific" papers full of their own presumptions, assumptions and suppositions about ME while ignoring the biological and biomedical evidence in over 5,000 research papers and ignoring the biomarkers for the abnormalities and dysfunctions found in ME. They then submitted these papers to scenitific and medical journals. Thus a process of misinformation and outright deception undermined scientific knowledge about this illness. They even tried to manipulate the World Health Organisation (WHO) to label ME as a psychiatric illness. This was done behind the scenes in a sly and devious manner.
(v) some psychiatrists used the fact that they published these "scientific" papers to apply for positions on government advisory committees and consultative committees for the NICE clinics and some have become so called "advisors" to the British, Danish, Dutch, Belgian, Swedish and US governments and health bodies. They then used their position to enforce their misguided views on other doctors, on civil servants and the government and the NICE clinics in relation to ME treatment (7). And they manipulated the civil servants and NICE clinics to ignore the biomedical and biological evidence from 5,000 research papers, detailing the physical abnormalities and dysfunctions and infections found in ME. All these NICE clinics offered was CBT and GET which were psychiatric treatments and did not improve patients or bring about recoveries (6,7). This enables some psychiatrists and psychologists to keep milking the system while depriving patients of much needed biological and biomedical based treatments, and wasting taxpayers money in the process.
(w) There have been several serious consequences for ME patients and their families arising from this hijacking of the illness by certain psychiatrists. The denial of proper medical diagnosis and identification of serious biological abnormalities and dysfunctions is one, denial of proper medical treatment is another, and the denial of research funding by governments and national health institutes and research institutes worldwide into the biological and biomedical aspects of ME is another. By calling ME an imaginary illness psychiatrists have undermined the credibility of ME and this has affected it's research funding from governments. Certain individuals in the NIH and CDC played a part in blocking funding for CFS research during this period, as they both thought it was not worth researching. From fiscal 1995 through fiscal 1997, some $5.8 million that the CDC told Congress had been spent on CFS research actually went to other activities. Certain members in the CDC tried to cover this up at the time. There were no criminal prosecutions and court cases at the time, and no one was fired or resigned, which was unusual when one considers the seriousness of the crimes and the fact that Americans were dying of the illness. Furthermore, Dr. Byron Hyde the famous Canadian doctor stated in his booklet ( A Brief History of Myalgic Encephalomyelitis ) that Dr. Straus (NIH) may have been responsible for misdirecting or misappropriating the $34 million designated by the US government for ME (CFS) research in the late 1980s' and 1990's. The $34 million was spent on researching other illnesses. This was a huge loss to ME (CFS) research.
While the Medical Research Council (MRC) in Britain was found to have had psychiatric bias in it's funding for ME research for over 10 years according to the findings of the Gibson Report (UK House of Parliament). In the case of the denial of research funding by governments and national health institutes and research institutes worldwide, it is estimated that certain psychiatrists have been responsible for denying $2 billion ($100 million x 20 years) in research funding into ME over 20 years. This $2 billion could have made a huge difference to scientific research and brought the world much closer to understanding the structure of causation of the illness and it's biological dynamics and led to the development of medical drugs to treat the illness.
The behaviour of some psychiatrists has been totally unacceptable and unethical. The views, the papers and the presumptions and assumptions of some psychiatrists in relation to ME need to be rejected by the scientific community and the medical community.
Videos about Insurance companies which denied disabled people their lawful payments. Some of these have advised governments. Some psychiatrists work as consultants, advisors, or executives for these insurance companies.
5. Carruthers M. Bruce, Jain Kumar Anil, De Meirleir L., Kenny, et. al. Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. 2003.
Carruthers M.,B., van de Sande I M, De Meirleir. L. K, et al. Myalgic encephalomyelitis: International Consensus Criteria. 2011.
6. Links to scientific and medical research papers below
8. Long-term Outcome of Cognitive Behavioural Therapy versus Relaxation Therapy for Chronic Fatigue Syndrome: A 5-Year Follow-Up Study. Alicia Deale, Trudie Chalder, Simon Wessely et al. Am J Psychiat 2001:158:2038-2042
6th AAME International Conference, Presentation by Dr Daniel Clauw. Study of 1,090 ME patients