Candida
overgrowth is common in ME patients. This fungus proliferates in
conditions of altered T-cell function and a weaknened immune system. It
affects the mouth, vagina and intestines. Since Candida is an
opportunistic fungus, attacking when the body is weak from illness such
as Cancer, HIV, Diabetes, Hepatitis, malnutrition, viral infections,
etc. or the immune system is weakened - this suggests that ME has
a significant effect on the immune system, very similar to that caused
by other chronic diseases.
Chester
AC.J Chronic Fatigue Syndrome 2000; 7: 87
High
rates of Candida infections have been found in CFS patients by Dr.
Paul Cheney. Dr. Paul Cheney is an international expert in CFS and
runs the Cheney Clinic in North Carolina, this clinic specialises in
treating CFS patients. http://fnmedcenter.com/ccis/
"The
most toxic entity in the body is candida or yeast. It is very
xenobiotic. When the liver is healthy it will clear these mycotoxins
through the urine. Therefore, we can test the urine for toxins to see
how the liver is functioning. Research from Australia has shown a
toxin called CFSUM-1 is found in the urine of CFS patients. Since then
many other toxins have been found, and they cause PAIN. The toxins
produced by candidiasis are Tartaric Acid and Arabinose. Cheney
described two boys diagnoses as autistic. When their urine was tested
they had high levels of Tartaric Acid and Arabinose. Both boys had
been on repeated antibiotics for recurring ear infections and had not
been autistic until recently. They were about six years old. Tartaric
Acid looks like Malic Acid and poisons cells by interferring with the
Krebs Cycle. Arabinose poisons the brain. When the two boys were
treated with nystatin for candidiasis they both recovered and were no
longer autistic."
Summary of a Lecture by Dr. Paul Cheney, MD, PhD May 7, 1998
The National CFIDS Foundation
103 Aletha Rd, Needham Ma 02492
(781) 449-3535 Fax (781) 449-8606
Cornell University, USA
Ongoing research (2016) by Professor Maureen Hanson — Liberty Hyde Bailey Professor, Department of Molecular and Genetics, Cornell University, New York, USA has found abnormally high levels of levels of lipopolysaccharides (LPS), as well as LBP and soluble CD14 (which are a natural consequence of high levels of LPS) in ME patients. They also found reduced levels of anti-inflammatory bacterial species (ruminococcae, which produce butyrate, an anti-inflammatory fatty acid) and species of bifidobacterium (which produce lactic acid) in ME/CFS patients. And with a combination of blood and gut tests they could identify 83% of sample correctly as coming from patients or controls. Tests are being developed to deliver 90 - 100% accuracy.
Sheedy JR,
Wettenhall RE, Scanion D, Gooley PR, Lewis DP, McGregor N, Stapleton DI, Butt HL, De Meirleir KL.
Increased D-lactic acid intestinal
bacteria in patients with chronic fatigue syndrome.
In Vivo
2009;
23:
621-8.
Sheedy JR, Wett
enhall RE, Scanlon D, Gooley PR, Lewis DP, McGregor N, et al.
Increased d
-
lactic acid intestinal bacteria in patients with chronic fatigue syndrome.
In
Vivo
(
2009
)
23
:
621
-
628.
Maes M, Mihaylova I, Leunis JC. Increased serum IgA and IgM against LPS of
ente
robacteria in chronic fatigue syndrome (CFS): indication for the involvement of
gram
-
negative enterobacteria in the etiology of CFS and for the presence of an
increased gut
-
intestinal permeability.
J Affect Disord
(
2007
)
99
:
237
-
240. doi:
10.1016/j.jad.200
6.08.021.
Frémont M, Coomans D, Massart S, de Meirleir K. High
-
throughput 16S rRNA gene
sequencing reveals alterations of intestinal microbiota in myalgic
encephalomyelitis/chronic fatigue syndrome patients.
Anaerobe
(
2013
)
22
:
50
-
56. doi:
10.1016/j.anaero
be.2013.06.002.
Lakhan SE, Kirchgessner A. Gut inflammation in chronic fatigue syndrome.
Nutr Metab
(Lond)
(2
010
)
7
:
79. doi: 10.1186/1743
-
7075
-
7
-
79.
De Meirleir KL, Khaiboullina SF, Frémont M, Hulstaert J, Rizvanov AA, Palotás A, et
al. Plasmacytoid dendr
itic cells in the duodenum of individuals diagnosed with myalgic
encephalomyelitis are uniquely immunoreactive to antibodies to human endogenous
retroviral proteins.
In Vivo
(2013)
27
:
177
-
187.
Maes M, Twisk FNM, Kubera M, Ringel K, Leunis JC, Geffard M. Increased IgA
responses to the LPS of commensal bacteria is associated with inflammation and
activation of cell
-
mediated immunity in chronic fatigue syndrome.
J Affect Disord
(
2012
)
136
:
909
-
917. doi:10.1016/j.jad.2011.09.010.
Maes M, Coucke F, Leunis JC: Normalization of the increased translocation of endotoxin from Gram negative enterobacteria (leaky gut) is accompanied by a remission of chronic fatigue syndrome. Neuro Endocrinol Lett 2007, 28:739-744.
IBS and Cognitive Problems
Altered cognitive function of prefrontal cortex during error feedback in patients with irritable bowel syndrome, based on FMRI and dynamic causal modeling.
Aizawa E, Sato Y, Kochiyama T, Saito N, Izumiyama M, Morishita J, Kanazawa M, Shima K, Mushiake H, Hongo M, Fukudo S.Gastroenterology. 2012 Nov;143(5):1188-98.
High histamine levels in the intestines can be caused by bad bacteria or intestinal dysbiosis. Histamine can increase inflammation in the gut and elsewhere in the body, reduce digestion and absorption and adversely affect the immune system and worsen the symptoms of ME. High histamine levels are commonly found in ME patients. It is a good indicator of intestinal dysbiosis.
The NIH in the USA has made some important new discoveries in relation to the intestines, microbiome and the immune system. They have found that the gut plays an important role in immune dysfunctions and abnormalities, the lymph system, and autoimmune illnesses.
(c)
The presence of Giardia parasites in ME patients
Giardia parasites have been found in a significant number of CFS
patients. These parasites can cause extreme tiredness, malabsorption of
food and nutrients, irritable bowel syndrome and allergies, which may
worsen the overall symptoms of Chronic Fatigue Syndrome.
Novotny,
T.E., et al. 1990. Prevalence of Giardia lamblia and risk factors
for infection among children attending day-care.. .Public Health
Reports 105:4, USA
Galland,
L. and Leem, M. 1990. Giardia lamblia infection as a cause of
chronic fatigue. Journal of Nutritional Medicine 1:27
"Another
consequence of poor intestinal integrity is fatigue resulting from
malabsorption of important nutrients. If the condition persists it
can lead to chronic fatigue syndrome. A giardia infection can be so
draining on the immune system that it causes fatigue. Again the
cause is often misdiag-nosed. A giardia epidemic in Placerville,
California, for example, was mysteriously followed by an epidemic of
chronic fatigue syndrome. In 1991 Dr. Galland and colleagues
published a study of 96 patients with chronic fatigue and
demonstrated active giardia infection in 46 percent. In another
study of 218 patients whose chief complaint was chronic fatigue, Dr.
Galland found that 61 patients were infected with giardia. His
conclusion is that giardia may be an important cause of chronic
fatigue syndrome."
"The Healing Miracles of Coconut Oil" by Bruce
Fife, ND.
(d)
Enteroviruses
Chronic fatigue syndrome is associated with chronic enterovirus infection of the stomach. John K S Chia, Andrew Y Chia.
J Clin Pathol 2007;0:1–6. doi: 10.1136/jcp.2007.050054
Acute enterovirus infection followed by myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and viral persistence.Chia J, Chia A, Voeller M, Lee T, Chang R.J.. Clin Pathol. 2010 Feb;63(2):165-8.
Dr. John Chia, is a world renowned doctor who has successfully treated ME / CFS patients. He has found that Enteroviruses are present in some subgroups of ME / CFS patients and that treating these Enterovirus infections can lead to significant improvement and recovery.
Dr. John Chia presents his findings up to the year 2011 to the National Institutes of Health (NIH) in the USA below:
Chronic Pelvic Pain (CPP) in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is Associated with Chronic Enterovirus Infection of Ovarian Tubes
John Chia, M.D., David Wang, Rabiha El-habbal and Andrew Chia, EV Med Research, Lomita California IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Pathogenesis of chronic enterovirus infection in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) –in vitro and in vivo studies of infected stomach tissuesJohn Chia, M.D., Andrew Chia, David Wang, Rabiha El-Habbal. EV Med Research. Lomita, CA. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Dowsett EG, Ramsay AM, McCartney RA, Bell EJ (1990), "Myalgic Encephalomyelitis (M.E.) -- A Persistent Enteroviral Infection?", Postgraduate Medical Journal, 66:526-530
Role of Infection and Neurologic Dysfunction in Chronic Fatigue Syndrome. Anthony L. Komaroff Tracey A. Cho. Semin Neurol 2011; 31(3): 325-337
Levine S (2001), "Prevalence in the cerebro spinal fluid of the following infectious agents in a cohort of 12 CFS subjects: Human Herpes Virus 6 & 8; Chlamydia Species; Mycoplasma Species, EBV; CMV and Coxsackie B Virus", Journal of Chronic Fatigue Syndrome, 9:91-2:41-51
“Enteroviral sequences were found in significantly more ME/CFS patients than in the two comparison groups….This study provides evidence for the involvement of enteroviruses in just under half of the patients presenting with ME/CFS and it confirms and extends previous studies using muscle biopsies. We provide evidence for the presence of viral sequences in serum in over 40% of ME/CFS patients” (J Med Virol 1995:45:156-161)
" Primary M.E. is always an acute onset illness. Doctors A. Gilliam, A.
Melvin Ramsay and Elizabeth Dowsett (who assisted
in much of his later work,) John Richardson of
Newcastle-upon-Tyne, W.H. Lyle, Elizabeth Bell of
Ruckhill Hospital, James Mowbray of St Mary's, and
Peter Behan all believed that the majority of primary
M.E. patients fell ill following exposure to an Enterovirus. (Poliovirus, ECHO, Coxsackie and the
numbered viruses are the significant viruses in this
group, but there are other enteroviruses that exist that
have been discovered in the past few decades that do
not appear in any textbook that I have perused.) I share
this belief that enteroviruses are a major cause. " Source:http://www.nightingale.ca/documents/Nightingale_ME_Definition_en.pdf
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810. 'Epidemic Neuromyasthenia' was used to describe ME in the past.
In the UK, about 60% of patients with ME / CFS have evidence of
enterovirus infection, most commonly Cocksackie B. This has been
demonstrated by the finding of enterovirus RNA in muscle and in blood.
Many other patients have reactivated Epstein Barr virus. It has not been
verified if the virus itself causes ME / CFS or it is the result of a
weakened immune system.
Source: Action for ME, Britain.
Enterovirus in the chronic fatigue syndrome. McGarry F, Gow J and Behan PO Ann Intern Med 1994:120:972 973
“Virological studies revealed that 76% of the patients with suspected myalgic encephalomyelitis had elevated Coxsackie B neutralising titres (and symptoms included) malaise, exhaustion on physical or mental effort, chest pain, palpitations, tachycardia, polyarthralgia, muscle pains, back pain, true vertigo, dizziness, tinnitus, nausea, diarrhoea, abdominal cramps, epigastric pain, headaches, paraesthesiae, dysuria)….The group described here are patients who have had this miserable illness. Most have lost many weeks of employment or the enjoyment of their family (and) marriages have been threatened…”
(BD Keighley, EJ Bell. JRCP 1983:33:339-341).
Levine S (2001), "Prevalence in the cerebro spinal fluid of the following infectious agents in a cohort of 12 CFS subjects: Human Herpes Virus 6 & 8; Chlamydia Species; Mycoplasma Species, EBV; CMV and Coxsackie B Virus", Journal of Chronic Fatigue Syndrome, 9:91-2:41-51
Gilliam AG (1938), "Epidemiological Study on an Epidemic, Diagnosed as Poliomyelitis, Occurring among the Personnel of Los Angeles County General Hospital during the Summer of 1934", United States Treasury Department Public Health Service Public Health Bulletin, No. 240, pp. 1-90. Washington, DC, Government Printing Office
During an outbreak of ME in Adelaide, Australia, in 1955, an agent (virus) was repeatedly transmitted to monkeys; when the monkeys were killed, microscopically, infiltration of nerve roots with lymphocytes and mononuclear cells was seen and some of the nerve fibres showed patchy damage in the myelin sheaths and axon swellings consistent with neurological involvement. In these monkeys, there were widespread changes involving the dorsal root ganglia, cervical and lumbar nerve roots and peripheral nerves. Perivascular collars of lymphocytes and plasma cells were in the cerebral cortex, brainstem and cerebellum, spinal cord and around blood vessels to nerve roots (Pellew RAA, Miles JAR; Med J Aust:1955:2:13:480-482, cited by J Gordon Parish; Postgraduate Medical Journal 1978:54:711-717). This research was cited by Dr. John Richardson in the British Medical Journal in 1978. These research findings have relevance, given the autopsy evidence presented at the Royal Society of Medicine meeting in the series “Medicine and me” on 11th July 2009 by Dr Abhijit Chaudhuri, where he showed slides of inflammation of the dorsal root ganglia in three ME/CFS patients.
Three
Babuska Clusters of Enteroviral-Associated Myalgic Encephalomyelitis
Nightingale
Research Foundation
Paper Presented by Byron Marshall Hyde M.D.
New South Wales, February 1998
Hickie I, et al. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. British Journal of Medicine 2006; 333 (7568):575.
"Myeloadenamate Deaminase deficiency in muscles of ME patients. It is
known that the enzyme is missing after a viral attack"
Professor Peter Behan, The Institute of Neurological Sciences,
University of Glasgow, Scotland.
“Recently associations have been found between Coxsackie B infection and a more chronic multisystem illness. A similar illness…has been referred to as… myalgic encephalomyelitis…140 patients presenting with symptoms suggesting a postviral syndrome were entered into the study…Coxsackie B antibody levels were estimated in 100 control patients…All the Coxsackie B virus antibody tests were performed blind…Of the 140 ill patients, 46% were found to be Coxsackie B virus antibody positive…This study has confirmed our earlier finding that there is a group of symptoms with evidence of Coxsackie B infection. We have also shown that clinical improvement is slow and recovery does not correlate with a fall in Coxsackie B virus antibody titre” (BD Calder et al. JRCGP 1987:37:11-14).
Presence of Viral Protein 1 (VP1)
"There are no tests to confirm a diagnosis, although 60% of sufferers will have a specific protein in their blood called viral protein 1, (VP1)."
Susan Clark, www.whatreallyworks.co.uk
Anti-pathogen and immune system treatments. Treatment of 741 italian patients with chronic fatigue syndrome. U. TIRELLI, A. LLESHI, M. BERRETTA, M. SPINA, R. TALAMINI, A. GIACALONE. European Review for Medical and Pharmacological Sciences 2013; 17: 2847-2852
Cunningham L, Bowles NE, Lane RJ, Dubowitz V, and Archard LC:
Persistence of Enteroviral RNA in Chronic Fatigue Syndrome is
Associated with the Abnormal Production of Equal Amounts of Positive
and Negative Strands of Enteroviral RNA. J General Virol 1990;
71:1399--1402
Findings and Testimony of Burke A. Cunha, MD., chief, infectious disease division, Winthrop-University Hospital, Mineola, N.Y., USA.
"But the most consistent lab evidence that we look for are elevations of coxsackie B-titers and elevations of HHV-6 titers in combination with the decrease in the percentage of natural killer T cells," Cunha explained.
"If the patient has two or three of these abnormalities in our study center, then he or she fits the laboratory criteria for chronic fatigue. Nearly all patients with crimson crescents have two out of three of these laboratory abnormalities," he said.
“These results show that chronic infection with enteroviruses occurs in many PVFS (post-viral fatigue syndrome, a classified synonym for ME/CFS) patients and that detection of enterovirus antigen in the serum is a sensitive and satisfactory method for investigating infection in these patients….Several studies have suggested that infection with enteroviruses is causally related to PVFS…The association of detectable IgM complexes and VP1 antigen in the serum of PVFS patients in our study was high…This suggests that enterovirus infection plays an important role in the aetiology of PVFS” (GE Yousef, EJ Bell, JF Mowbray et al. Lancet January 23rd 1988:146-150).
Prevalence in the cerebrospinal fluid of the following infectious agents in a cohort of 12 CFS subjects: human herpes virus 6 and 8; chlamydia species; mycoplasma species;
EBV; CMV; and coxsackie virus. Journal of Chronic Fatigue Syndrome, 2001, 9, 1/2, 41-51
Viral Infection in CFS patients. The Clinical and Scientific Basis
of ME / CFS, Byron M. Hyde M.D., Ed., The Nightingale Research
Foundation, 1992, 325-327.
“Myalgic encephalomyelitis is a common disability but frequently misinterpreted…This illness is distinguished from a variety of other post-viral states by a unique clinical and epidemiological pattern characteristic of enteroviral infection…33% had titres indicative and 17% suggestive of recent CBV infection…Subsequently…31% had evidence of recent active enteroviral infection…There has been a failure to recognise the unique epidemiological pattern of ME…Coxsackie viruses are characteristically myotropic and enteroviral genomic sequences have been detected in muscle biopsies from patients with ME. Exercise related abnormalities of function have been demonstrated by nuclear magnetic resonance and single-fibre electromyography including a failure to coordinate oxidative metabolism with anaerobic glycolysis causing abnormal early intracellular acidosis, consistent with the early fatiguability and the slow recovery from exercise in ME. Coxsackie viruses can initiate non-cytolytic persistent infection in human cells. Animal models demonstrate similar enteroviral persistence in neurological disease… and the deleterious effect of forced exercise on persistently infected muscles. These studies elucidate the exercise-related morbidity and the chronic relapsing nature of ME” (EG Dowsett, AM Ramsay et al. Postgraduate Medical Journal 1990:66:526-530).
“The findings described here provide the first evidence that postviral fatigue syndrome may be due to a mitochondrial disorder precipitated by a virus infection…Evidence of mitochondrial abnormalities was present in 80% of the cases with the commonest change (seen in 70%) being branching and fusion of cristae, producing ‘compartmentalisation’. Mitochondrial pleomorphism, size variation and occasional focal vacuolation were detectable in 64%…Vacuolation of mitochondria was frequent…In some cases there was swelling of the whole mitochondrion with rupture of the outer membranes…prominent secondary lysosomes were common in some of the worst affected cases…The pleomorphism of the mitochondria in the patients’ muscle biopsies was in clear contrast to the findings in normal control biopsies…Diffuse or focal atrophy of type II fibres has been reported, and this does indicate muscle damage and not just muscle disuse” (WMH Behan et al. Acta Neuropathologica 1991:83:61-65).
“Persistent enteroviral infection of muscle may occur in some patients with postviral fatigue syndrome and may have an aetiological role….The features of this disorder suggest that the fatigue is caused by involvement of both muscle and the central nervous system…We used the polymerase chain reaction to search for the presence of enteroviral RNA sequences in a well-characterised group of patients with the postviral fatigue syndrome…53% were positive for enteroviral RNA sequences in muscle…Statistical analysis shows that these results are highly significant…On the basis of this study…there is persistent enteroviral infection in the muscle of some patients with the postviral fatigue syndrome and this interferes with cell metabolism and is causally related to the fatigue” (JW Gow et al. BMJ 1991:302:696-696).
“Postviral fatigue syndrome / myalgic encephalomyelitis… has attracted increasing attention during the last five years…Its distinguishing characteristic is severe muscle fatiguability made worse by exercise…The chief organ affected is skeletal muscle, and the severe fatiguability, with or without myalgia, is the main symptom. The results of biochemical, electrophysiological and pathological studies support the view that muscle metabolism is disturbed, but there is no doubt that other systems, such as nervous, cardiovascular and immune are also affected…Recognition of the large number of patients affected…indicates that a review of this intriguing disorder is merited….The true syndrome is always associated with an infection…Viral infections in muscle can indeed be associated with a variety of enzyme abnormalities…(Electrophysiological results) are important in showing the organic nature of the illness and suggesting that muscle abnormalities persist after the acute infection…there is good evidence that Coxsackie B virus is present in the affected muscle in some cases” (PO Behan, WMH Behan. CRC Crit Rev Neurobiol 1988:4:2:157-178).
“The main features (of ME) are: prolonged fatigue following muscular exercise or mental strain, an extended relapsing course; an association with neurological, cardiac, and other characteristic enteroviral complications. Coxsackie B neutralisation tests show high titres in 41% of cases compared with 4% of normal adults…These (chronic enteroviral syndromes) affect a young, economically important age group and merit a major investment in research” (EG Dowsett. Journal of Hospital Infection 1988:11:103-115).
“Ten patients with post-viral fatigue syndrome and abnormal serological, viral, immunological and histological studies were examined by single fibre electromyographic technique….The findings confirm the organic nature of the disease. A muscle membrane disorder…is the likely mechanism for the fatigue and the single-fibre EMG abnormalities. This muscle membrane defect may be due to the effects of a persistent viral infection…There seems to be evidence of a persistent viral infection and/or a viral-induced disorder of the immune system…The infected cells may not be killed but become unable to carry out differentiated or specialised function” (Goran A Jamal, Stig Hansen. Euro Neurol 1989:29:273-276).
“Molecular viral studies have recently proved to be extremely useful. They have confirmed the likely important role of enteroviral infections, particularly with Coxsackie B virus” (Postviral fatigue syndrome: Current neurobiological perspective. PGE Kennedy. BMB 1991:47:4:809-814)
In his Summary of the Viral Studies of CFS, Dr Dharam V Ablashi concluded: “The presentations and discussions at this meeting strongly supported the hypothesis that CFS may be triggered by more than one viral agent…Komaroff suggests that, once reactivated, these viruses contribute directly to the morbidity of CFS by damaging certain tissues and indirectly by eliciting an on-going immune response”(Clin Inf Dis 1994:18 (Suppl 1):S130-133). It is recommended that the entire 167-page Journal be read
“Our focus will be on the ability of certain viruses to interfere subtly with the cell’s ability to produce specific differentiated products as hormones, neurotransmitters, cytokines and immunoglobulins etc in the absence of their ability to lyse the cell they infect. By this means viruses can replicate in histologically normal appearing cells and tissues…Viruses by this means likely underlie a wide variety of clinical illnesses, currently of unknown aetiology, that affect the endocrine, immune, nervous and other …systems” (JC de la Torre, P Borrow, MBA Oldstone. BMB 1991:47:4:838-851).
“We conclude that persistent enteroviral infection plays a role in the pathogenesis of PVFS…The strongest evidence implicates Coxsackie viruses…Patients with PVFS were 6.7 times more likely to have enteroviral peristence in their muscles” (JW Gow and WMH Behan. BMB 1991:47:4:872-885).
“The postviral fatigue syndrome (PVFS), with profound muscle fatigue on exertion and slow recovery from exhaustion seems to be related specifically to enteroviral infection. The form seen with chronic reactivated EBV infection is superficially similar, but without the profound muscle fatigue on exercise” (JF Mowbray, GE Yousef. BMB 1991:47:4:886-894).
“Skeletal samples were obtained by needle biopsy from patients diagnosed clinically as having CFS (and) most patients fulfilled the criteria of the Centres for Disease Control for the diagnosis of CFS (Holmes et al 1988)…These data are the first demonstration of persistence of defective virus in clinical samples from patients with CFS…We are currently investigating the effects of persistence of enteroviral RNA on cellular gene expression leading to muscle dysfunction” (L Cunningham, RJM Lane, LC Archard et al. Journal of General Virology 1990:71:6:1399-1402).
“These results suggest there is persistence of enterovirus infection in some CFS patients and indicate the presence of distinct novel enterovirus sequences…Several studies have shown that a significant proportion of patients complaining of CFS have markers for enterovirus infection….From the data presented here…the CFS sequences may indicate the presence of novel enteroviruses…It is worth noting that the enteroviral sequences obtained from patients without CFS were dissimilar to the sequences obtained from the CFS patients…This may provide corroborating evidence for the presence of a novel type of enterovirus associated with CFS” (DN Galbraith, C Nairn and GB Clements. Journal of General Virology 1995:76:1701-1707).
“We will report at the First International Research Conference on Chronic Fatigue Syndrome to be held at Albany, New York, 2-4 October 1992, our new findings relating particularly to enteroviral infection…We have isolated RNA from patients and probed this with large enterovirus probes…detailed studies...showed that the material was true virus…Furthermore, this virus was shown to be replicating normally at the level of transcription. Sequence analysis of this isolated material showed that it had 80% homology with Coxsackie B viruses and 76% homology with poliomyelitis virus, demonstrating beyond any doubt that the material was enterovirus” (Press Release for the Albany Conference, Professor Peter O Behan, University of Glasgow, October 1992).
“In the CFS study group, 42% of patients were positive for enteroviral sequences by PCR, compared to only 9% of the comparison group…Enteroviral PCR does, however, if positive, provide evidence for circulating viral sequences, and has been used to show that enteroviral specific sequences are present in a significantly greater proportion of CFS patients than other comparison groups” (C Nairn et al. Journal of Medical Virology 1995:46:310-313).
“Samples from 25.9% of the PFS (postviral fatigue syndrome) were positive for the presence of enteroviral RNA, compared with only 1.3% of the controls…We propose that in PFS patients, a mutation affecting control of viral RNA synthesis occurs during the initial phase of active virus infection and allows persistence of replication defective virus which no longer attracts a cellular immune response” (NE Bowles, RJM Lane, L Cunningham and LC Archard. Journal of Medicine 1993:24:2&3:145-180).
“These data support the view that while there may commonly be asyptomatic enterovirus infections of peripheral blood, it is the presence of persistent virus in muscle which is abnormal and this is associated with postviral fatigue syndrome…Evidence derived from epidemiological, serological, immunological, virological, molecular hybridisation and animal experiments suggests that persistent enteroviral infection may be involved in… PFS” (PO Behan et al. CFS: CIBA Foundation Symposium 173, 1993:146-159).
Seeking to detect and characterise enterovirus RNA in skeletal muscle from patients with (ME)CFS and to compare efficiency of muscle metabolism in enterovirus positive and negative (ME)CFS patients, Lane et al obtained quadriceps biopsy samples from 48 patients with (ME)CFS. Muscle biopsy samples from 20.8% of patients were positive, while 100% of the controls were negative for enterovirus sequences. Lane et al concluded: “There is an association between abnormal lactate response to exercise, reflecting impaired muscle energy metabolism, and the presence of enterovirus sequences in muscle in a proportion of (ME)CFS patients” (RJM Lane, LC Archard et al. JNNP 2003:74:1382-1386).
Kerr et al then go on to provide evidence of other triggers of (ME)CFS which include Parvovirus; C. pneumoniae; C. burnetti; toxin exposure and vaccination including MMR, pneumovax, influenza, hepatitis B, tetanus, typhoid and poliovirus (LD Devanur, JR Kerr. Journal of Clinical Virology 2006: 37(3):139-150).
“Research studies have identified various features relevant to the pathogenesis of CFS/ME such as viral infection, immune abnormalities and immune activation, exposure to toxins, chemicals and pesticides, stress, hypotension…and neuroendocrine dysfunction….Various viruses have been shown to play a triggering or perpetuating role, or both, in this complex disease….The role of enterovirus infection as a trigger and perpetuating factor in CFS/ME has been recognised for decades…The importance of gastrointestinal symptoms in CFS/ME and the known ability of enteroviruses to cause gastrointestinal infections led John and Andrew Chia to study the role of enterovirus infection in the stomach of CFS/ME patients…They describe a systematic study of enterovirus infection in the stomach of 165 CFS/ME patients, demonstrating a detection rate of enterovirus VP1 protein in 82% of patients…the possibility of an EV outbreak…seems unlikely, as these patients developed their diseases at different times over a 20 year period” (Jonathan R Kerr. Editorial. J Clin Pathol 14th September 2007. Epub ahead of print).
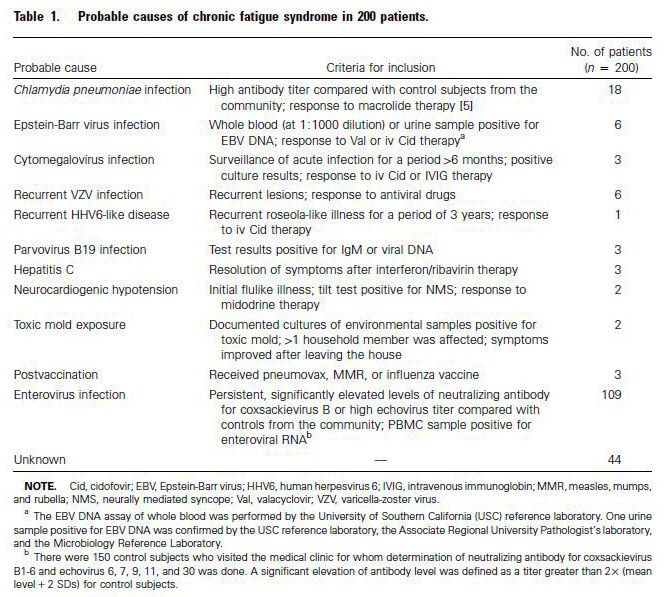
“Since most (ME)CFS patients have persistent or intermittent gastrointestinal (GI) symptoms, the presence of viral capsid protein 1 (VP1), enterovirus RNA and culturable virus in the stomach biopsy specimens of patients with (ME)CFS was evaluated…Our recent analysis of 200 patients suggests that… enteroviruses may be the causative agents in more than half of the patients…At the time of oesophagogastroduodenoscopy, the majority of patients had mild, focal inflammation in the antrum…95% of biopsy specimens had microscopic evidence of mild chronic inflammation…82% of biopsy specimens stained positive for VP1 within parietal cells, whereas 20% of the controls stained positive…An estimated 80-90% of our 1,400 (ME)CFS patients have recurring gastrointestinal symptoms of varying severity, and epigastric and/or lower quadrant tenderness by examination…Finding enterovirus protein in 82% of stomach biopsy samples seems to correlate with the high percentage of (ME)CFS patients with GI complaints…Interestingly, the intensity of VP1 staining of the stomach biopsy correlated inversely with functional capacity…A significant subset of (ME)CFS patients may have a chronic, disseminated, non-cytolytic form of enteroviral infection which can lead to diffuse symptomatology without true organ damage” (Chia JK, Chia AY. J Clin Pathol 13th September 2007 Epub ahead of print).
In a review of the role of enteroviruses in (ME)CFS, Chia noted that initial reports of chronic enteroviral infections causing debilitating symptoms in (ME)CFS patients were met with scepticism and largely forgotten, but observations from in vitro experiments and from animal models clearly established a state of chronic persistence through the formation of double stranded RNA, similar to findings reported in muscle biopsies of patients with (ME)CFS. Recent evidence not only confirmed the earlier studies, but also clarified the pathogenic role of viral RNA (JKS Chia. Journal of Clinical Pathology 2005:58:1126-1132).
Torrisi, et al, wrote "The absence of lycoproteins on the cell
surface of the infected cells," showing where the virus is hiding
and how it infects (Virology, 257, 1999).
Detection of Viral Related Sequences in CFS Patients Using the
Polymerase Chain Reaction. The Clinical and Scientific Basis of ME /
CFS, Byron M. Hyde M.D., Ed., The Nightingale Research Foundation,
1992, 278-282.
As mentioned elsewhere, researchers from the Enterovirus Research Laboratory, Department of Pathology and Microbiology, University of Nebraska Medical Centre wrote a specially-commissioned explanatory article for the UK charity Invest in ME, in which they stated that human enteroviruses were not generally thought to persist in the host after an acute infection, but they had discovered that Coxsackie B viruses can naturally delete sequence from the 5’ end of the RNA genome, and that this results in long-term viral persistence, and that “This previously unknown and unsuspected aspect of enterovirus replication provides an explanation for previous reports of enteroviral RNA detected in diseased tissue in the apparent absence of infectious virus particles” (S Tracy and NM Chapman. Journal of IiME 2009:3:1).
(http://www.investinme.org/Documents/Journals/Journal%20of%20IiME%20Vol%203%20Issue%201.pdf).
“Recent developments in molecular biology…have revealed a hitherto unrecognised association between enteroviruses and some of the most disabling, chronic and disheartening neurological, cardiac and endocrine diseases…Persistent infection (by enteroviruses) is associated with ME/CFS…The difficulty of making a differential diagnosis between ME/CFS and post-polio sequelae cannot be over-emphasised…(EG Doswett. Commissioned for the BASEM meeting at the RCGP, 26th April 1998:1-10).
“To prove formally that persistence rather than re-infection is occurring, it is necessary to identify a unique feature retained by serial viral isolates from one individual. We present here for the first time evidence for enteroviral persistence (in humans with CFS)…” (DN Galbraith et al. Journal of General Virology 1997:78:307-312).