The International Consensus Criteria (2011) is very clear about the harmful effects of exercise, and physical exertion and mental exertion. It uses the term Post- Exertional Neuroimmune Exhaustion (PENE) to define the harmful effects of physical exertion or mental exertion, and the abnormal severe exhausation after physical activity or mental activity, and that this indicates the effects of a disease process. ME Primer for Healthcare Professionals: based on Myalgic encephalomyelitis: International Consensus Criteria, 2012
The Canadian Criteria (2003) is very definite in it's statements about the harmful effects of exercise, and physical exertion and mental exertion. It uses a term Post Exercise Malaise (PEM) to describe the abnormal severe exhaustion from physical exercise or mental exercise and the harmful effects of exercise. It believes that this is part of a disease process.
The new name SEID created by the IOM of the US National Academies of Science in 2015 means 'Systemic Exertion Intolerance Disease'. The name and defintion point to the fact that there is exertion or exercise intolerance in this disease. It accepts Post Exertional Malaise (PEM) as being part of the disease, and that physical exertion or mental exertion can cause harmful effects in ME patients. It accepts that there is a disease process causing this. The IOM defintion states that it is “a disease characterized by profound fatigue, cognitive dysfunction, sleep abnormalities, autonomic manifestations, pain, and other symptoms that are made worse by exertion of any sort. ME/CFS can severely impair patients’ ability to conduct their normal lives.”
This corroborates findings from the Canadian Criteria (2003) and the International Consensus criteria 2011 shown above.
US National Academies of Science, Institute of Medicine report: "Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness" 2015 http://iom.nationalacademies.org/Reports/2015/ME-CFS.aspx
Redefining the Chronic Fatigue Syndrome, Professor Theodore G. Ganiats MD, Ann Intern Med.2015;162(9):653-654. http://dx.doi.org/10.7326/M15-0357 in response to SEID criteria stated the following in 2015:
"This message should reassure the millions of people with the condition that their concerns are, indeed, legitimate, while sounding a wake-up call to clinicians and research funders that ME/CFS deserves closer attention."
"Other key findings (SEID) .......postexertional malaise, where exertion from activity (even seemingly mild activity, such as walking or active cognition) can trigger a “collapse” or “relapse” of malaise that lasts days or longer, far in excess of what would normally be expected. There may be a delay between the trigger and the collapse. Physiologic abnormalities after exertion are seen, which supports patient reports that forcing a person to “push” themselves can lead to profound exacerbation of symptoms."
"These new criteria (SEID) highlight the critical importance of postexertional malaise, which is so characteristic that the committee believes that the concept of exertion intolerance should be part of a new name."
[Fatiguability]: Muscle fatigability, whereby, even after a minor degree of physical effort, three, four or five days, or longer, elapse before full muscle power is restored and constitutes the sheet anchor of diagnosis. Without it I would be unwilling to diagnose a patient as suffering from ME, but it is most important to stress the fact that cases of ME or mild or even moderate severity may have normal muscle power in a remission. In such cases, tests for muscle power should be repeated after exercise.
Metabolic dysfunction causes Post-Exertional malaise in ME/CFS Staci R. Stevens, MA, and Christopher Snell, Ph.D:
Staci R. Stevens, MA, Executive Director
Pacific Fatigue Laboratory
University of the Pacific
sstevens@pacific.edu
Christopher Snell, Ph.D
Department Chair
Exercise & Sport Sciences
University of the Pacific
csnell@pacific.edu
Loss of capacity to recover from acidosis on repeat exercise in chronic fatigue syndrome: a case-control study. Jones DE, Hollingsworth KG, Jakovljevic DG, Fattakhova G, Pairman J, Blamire AM, Trenell MI, Newton JL. Eur J Clin Invest. 2012 Feb;42(2):186-94
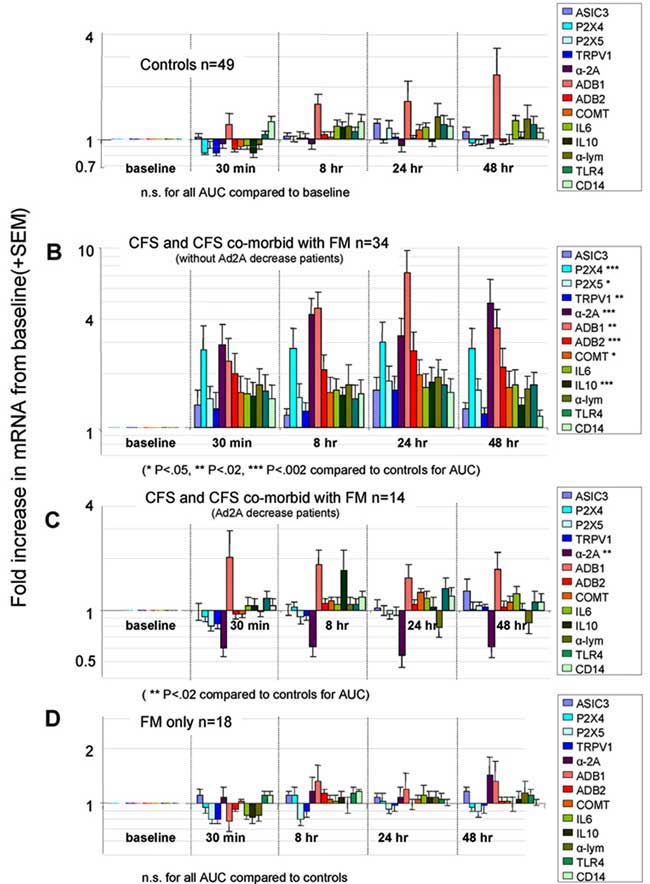
Abnormally changed genes associated with the following biological pathways and proteins after exercise have been linked to CFS according to studies conducted by Dr. Light in the University of Utah, USA:
There is significant and continuing abnormalities in these genes and receptors after exercise.according to studies conducted by Dr. Light in Utah. See Scientific Evidence Section - Genetic Markers
Source: Moderate Exercise Increases Expression for Sensory, Adrenergic, and Immune Genes in Chronic Fatigue Syndrome Patients But Not in Normal Subjects
Alan R. Lightemail address
,
Andrea T. White
,
Ronald W. Hughen
,
Kathleen C. Light. The Journal of Pain
Volume 10, Issue 10 , Pages 1099-1112, October 2009.
VanNess JM, Snell CR, Stevens SR, Diminished cardiopulmonary capacity during post-exertional malaise in chronic fatigue syndrome. JCFS 2007; 14. 77-85
Time course of exercise induced alterations in daily activity in chronic fatigue syndrome. Christopher D Black and Kevin K McCully. Dynamic Medicine 2005, 4:10
Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2 peak indicates functional impairment
Betsy A Keller, John Luke Pryor and Ludovic Giloteaux
Journal of Translational Medicine 2014
Vermeulen RC, W VvEI. Decreased oxygen extraction during cardiopulmonary
exercise test in patients with chronic fatigue
syndrome.
J Transl Med
(
2014
)
12
:
20.
Dysfunctional Endogenous Analgesia During Exercise in Patients with Chronic Pain: To Exercise or Not to Exercise? Nijs et al. Pain Physician 2012; 15:ES205-ES213
Twisk FN, Maes M. Chronic fatigue syndrome: Harvey and Wessely's (bio)psychosocial model versus a bio(psychosocial) model based on inflammatory and oxidative and nitrosative stress pathways. 2010.
Twisk FN, Maes M. A review on cognitive behavorial therapy (CBT) and graded exercise therapy (GET) in myalgic encephalomyelitis (ME) / chronic fatigue syndrome (CFS): CBT/GET is not only ineffective and not evidence-based, but also potentially harmful for many patients with ME/CFS. Neuro Endocrin lett. 2009, 30(3): 284-299.
Some recent research into CBT, GET and Pacing in Britain in 2015 contradicts the PACE findings. Of patients who received GET, 74 percent said that it had made them worse. While 18 percent said they were worse after cognitive behavior therapy and only 14 percent after pacing.
Christopher R. Snell, Staci R. Stevens, Todd E. Davenport and J. Mark VanNess (2013). Discriminative Validity
of Metabolic and Workload Measurements to Identify Individuals with Chronic Fatigue Syndrome. PHYS THER. Published online June 27, 2013 doi: 10.2522/ptj.20110368
Discriminative Validity of Metabolic and Workload Measurements to Identify Individuals With Chronic Fatigue Syndrome.
Snell CR, Stevens SR, Davenport TE, Van Ness JM. Phys Ther. 2013
Núñez M, Fernández-Solà J, Nuñez E, Fernández-Huerta JM, Godás-Sieso T, Gomez-Gil E. Health-related quality of life in patients with chronic fatigue syndrome: group cognitive behavioural therapy and graded exercise versus usual treatment. A randomised controlled trial with 1 year of follow-up. Clin Rheumatol. 2011.
Video interviews with Dr. Alan Light, genetic scientist
Abnormalities of AMPK Activation and glucose uptake in cultured skeletal muscle cells from individuals with chronic fatigue syndrome.
Brown AE, Jones DE, Walker M, Newton JL. Plos One 2015
Maureen Hanson (New York,USA) presented research findings on exercise, VO2 and ME at the International ME Conference 2014"CPET using a bike with resistance showed on a 2nd test 24 hours later that CPET values could not be reproduced in ME patients. In other diseases patients can usually reproduce their base response 24 hours later...............ME patients showed a 25% decrease on VO2 max on second day. In patients who also have dysautonomia, the BP does not go up and they have to stop. Subgroups have been detected also in the 2nd CPET, which may correlate with signalling molecules in the blood. There are changes in chemokines and cytokines. 10 cytokines were measured and 5 were decreased markedly. A pilot study compared metabolites in ME patients and found 52 significant differences between before CPET1 and after CPET2. There was reduction in several acylcarnitines after exercise. 300 polar metabolites were examined and 83 differed significantly. Most were higher in controls than patients. Acetyl-carnosine was 2-fold lower in patients than controls.In conclusion: ME patients cannot reproduce their performance on a 2nd CPET. The abnormal responses can affect the autonomic or physiological responses to exercise"
L.
Paul, WHM Behan, WM McLaren. Demonstration of delayed recovery from
fatiguing exercise in CFS. Eur. J. Neurology 1999, 6, 63-69)
There is mounting evidence that oxidative stress and, more specifically, lipid peroxidation,
contribute to the disease process and to some of the symptoms in (ME/CFS). The novel findings
in this study are that patients with (ME)CFS have sig
nificantly elevated levels
of F
2
of F2
isoprostanes alongside other key markers of oxidative stress and that these correlate with various
(ME)CFS symptoms. This is the first time that elevated levels of isoprostanes have been reported
in patients with (M
E)CFS. Isoprostanes have been shown to be powerfully vasoconstricting and
are involved in endothelial injury. Research has demonstrated that incremental exercise
challenge potentiates a prolonged and accentuated oxidant stress that might well account for
p
ostexercise symptoms in (ME)CFS patients. It could be suggested that (ME)CFS is an
inflammatory condition (which) could explain many of the pathological manifestations that
underlie the illness".
Oxidative stress levels are raised in chronic fatigue synd
rome and are
associated with clinical symptoms. Gwen Kennedy, Vance Spence et al. Free Radical Biology and
Medicine: 2005:39:584
-
589
Jammes Y, Steinberg JG, Mambrini O, et al. 2005 Chronic fatigue syndrome: assessment of increased oxidative stress and altered muscle excitability in response to incremental exercise. J Intern Med 257:299-310.
Superior Ability of a Two-Day CPET Protocol to Detect Functional Impairment in ME/CFS Compared to Either a Single CPET, A Submaximal Exercise Test, or a VO2 Prediction Equation. Betsy A. Keller, Ithaca College, Dept. of Exercise and Sport Sciences, Ithaca NY IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Diminished Pulmonary Ventilation in CFS Patients – Effects of Deconditioning and Post-Exertional Malaise. J. Mark VanNess, Ph.D. Associate Professor, University of the Pacific. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO₂peak indicates functional impairment. Keller et al. J Transl Med. 2014 Apr 23;12:104.
"ME/CFS patients showed significant decreases from CPET1 to CPET2 in VO₂peak (13.8%), HRpeak (9 bpm), Ve peak (14.7%), and Work@peak (12.5%). Decreases in VT measures included VO₂@VT (15.8%), Ve@VT (7.4%), and Work@VT (21.3%). Peak RER was high (≥1.1) and did not differ between tests, indicating maximum effort by participants during both CPETs. If data from only a single CPET test is used, a standard classification of functional impairment based on VO₂peak or VO @VT results in over-estimation of functional ability for 50% of ME/CFS participants in this study."
Oxygen Extraction and Lactate Are Low during Cardiopulmonary Exercise Test in Patients with Chronic Fatigue Syndrome
RCW Vermeulen, WG Vermeulen – van Eck and I.V. de Jong – Medvetska Head of Research, CVS Centrum Amsterdam. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Specific Fitness Profile to Effort in CFS
Alegre J, Suarez A, García-Quintana AM, Castro-Marrero J, García-Quintana J.
Chronic Fatigue Group. Vall d´Hebron University Hospital Research Institute. Universidad Autónoma de Barcelona. Spain. 2CFS Unit. Centro Médico Delfos. Barcelona. Spain IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Intracellular generation of reactive oxygen species by contracting skeletal muscle cells.
McArdle F, Pattwell DM, Vasilaki A, McArdle A, Jackson MJ
Free Radic Biol Med. 2005 Sep 1; 39(5):651-7.
Lane RJ, Burgess AP, Flint J, Riccio M, Archard LC. Exercise responses and psychiatric disorder in chronic fatigue syndrome. BMJ 1995 Aug;311(7004):544-545.
Lane RJ, Barrett MC, Woodrow D, Moss J, Fletcher R, Archard LC. Muscle fibre characteristics and lactate responses to exercise in chronic fatigue syndrome. J Neurol Neurosurg Psychia 1998 Mar;64(3):362-367.
“The pleomorphism of the mitochondria in the patients’ muscle biopsies was in clear contrast to the findings in the normal control biopsies. Diffuse or focal atrophy of type II fibres has been reported, and this does indicate muscle damage and not just muscle disuse”. (Acta Neuropathol 1991:83:61-65).
“Myalgic encephalomyelitis is a common disability but frequently misinterpreted…This illness is distinguished from a variety of other post-viral states by a unique clinical and epidemiological pattern characteristic of enteroviral infection…33% had titres indicative and 17% suggestive of recent CBV infection…Subsequently…31% had evidence of recent active enteroviral infection…There has been a failure to recognise the unique epidemiological pattern of ME…Coxsackie viruses are characteristically myotropic and enteroviral genomic sequences have been detected in muscle biopsies from patients with ME. Exercise related abnormalities of function have been demonstrated by nuclear magnetic resonance and single-fibre electromyography including a failure to coordinate oxidative metabolism with anaerobic glycolysis causing abnormal early intracellular acidosis, consistent with the early fatiguability and the slow recovery from exercise in ME. Coxsackie viruses can initiate non-cytolytic persistent infection in human cells. Animal models demonstrate similar enteroviral persistence in neurological disease… and the deleterious effect of forced exercise on persistently infected muscles. These studies elucidate the exercise-related morbidity and the chronic relapsing nature of ME” (EG Dowsett, AM Ramsay et al. Postgraduate Medical Journal 1990:66:526-530).
“The findings described here provide the first evidence that postviral fatigue syndrome may be due to a mitochondrial disorder precipitated by a virus infection…Evidence of mitochondrial abnormalities was present in 80% of the cases with the commonest change (seen in 70%) being branching and fusion of cristae, producing ‘compartmentalisation’. Mitochondrial pleomorphism, size variation and occasional focal vacuolation were detectable in 64%…Vacuolation of mitochondria was frequent…In some cases there was swelling of the whole mitochondrion with rupture of the outer membranes…prominent secondary lysosomes were common in some of the worst affected cases…The pleomorphism of the mitochondria in the patients’ muscle biopsies was in clear contrast to the findings in normal control biopsies…Diffuse or focal atrophy of type II fibres has been reported, and this does indicate muscle damage and not just muscle disuse” (WMH Behan et al. Acta Neuropathologica 1991:83:61-65).
“Persistent enteroviral infection of muscle may occur in some patients with postviral fatigue syndrome and may have an aetiological role….The features of this disorder suggest that the fatigue is caused by involvement of both muscle and the central nervous system…We used the polymerase chain reaction to search for the presence of enteroviral RNA sequences in a well-characterised group of patients with the postviral fatigue syndrome…53% were positive for enteroviral RNA sequences in muscle…Statistical analysis shows that these results are highly significant…On the basis of this study…there is persistent enteroviral infection in the muscle of some patients with the postviral fatigue syndrome and this interferes with cell metabolism and is causally related to the fatigue” (JW Gow et al. BMJ 1991:302:696-696).
“Postviral fatigue syndrome / myalgic encephalomyelitis… has attracted increasing attention during the last five years…Its distinguishing characteristic is severe muscle fatiguability made worse by exercise…The chief organ affected is skeletal muscle, and the severe fatiguability, with or without myalgia, is the main symptom. The results of biochemical, electrophysiological and pathological studies support the view that muscle metabolism is disturbed, but there is no doubt that other systems, such as nervous, cardiovascular and immune are also affected…Recognition of the large number of patients affected…indicates that a review of this intriguing disorder is merited….The true syndrome is always associated with an infection…Viral infections in muscle can indeed be associated with a variety of enzyme abnormalities…(Electrophysiological results) are important in showing the organic nature of the illness and suggesting that muscle abnormalities persist after the acute infection…there is good evidence that Coxsackie B virus is present in the affected muscle in some cases” (PO Behan, WMH Behan. CRC Crit Rev Neurobiol 1988:4:2:157-178).
“The main features (of ME) are: prolonged fatigue following muscular exercise or mental strain, an extended relapsing course; an association with neurological, cardiac, and other characteristic enteroviral complications. Coxsackie B neutralisation tests show high titres in 41% of cases compared with 4% of normal adults…These (chronic enteroviral syndromes) affect a young, economically important age group and merit a major investment in research” (EG Dowsett. Journal of Hospital Infection 1988:11:103-115).
“Ten patients with post-viral fatigue syndrome and abnormal serological, viral, immunological and histological studies were examined by single fibre electromyographic technique….The findings confirm the organic nature of the disease. A muscle membrane disorder…is the likely mechanism for the fatigue and the single-fibre EMG abnormalities. This muscle membrane defect may be due to the effects of a persistent viral infection…There seems to be evidence of a persistent viral infection and/or a viral-induced disorder of the immune system…The infected cells may not be killed but become unable to carry out differentiated or specialised function” (Goran A Jamal, Stig Hansen. Euro Neurol 1989:29:273-276).
“Molecular viral studies have recently proved to be extremely useful. They have confirmed the likely important role of enteroviral infections, particularly with Coxsackie B virus” (Postviral fatigue syndrome: Current neurobiological perspective. PGE Kennedy. BMB 1991:47:4:809-814)
In his Summary of the Viral Studies of CFS, Dr Dharam V Ablashi concluded: “The presentations and discussions at this meeting strongly supported the hypothesis that CFS may be triggered by more than one viral agent…Komaroff suggests that, once reactivated, these viruses contribute directly to the morbidity of CFS by damaging certain tissues and indirectly by eliciting an on-going immune response”(Clin Inf Dis 1994:18 (Suppl 1):S130-133). It is recommended that the entire 167-page Journal be read
“Our focus will be on the ability of certain viruses to interfere subtly with the cell’s ability to produce specific differentiated products as hormones, neurotransmitters, cytokines and immunoglobulins etc in the absence of their ability to lyse the cell they infect. By this means viruses can replicate in histologically normal appearing cells and tissues…Viruses by this means likely underlie a wide variety of clinical illnesses, currently of unknown aetiology, that affect the endocrine, immune, nervous and other …systems” (JC de la Torre, P Borrow, MBA Oldstone. BMB 1991:47:4:838-851).
“We conclude that persistent enteroviral infection plays a role in the pathogenesis of PVFS…The strongest evidence implicates Coxsackie viruses…Patients with PVFS were 6.7 times more likely to have enteroviral peristence in their muscles” (JW Gow and WMH Behan. BMB 1991:47:4:872-885).
“The postviral fatigue syndrome (PVFS), with profound muscle fatigue on exertion and slow recovery from exhaustion seems to be related specifically to enteroviral infection. The form seen with chronic reactivated EBV infection is superficially similar, but without the profound muscle fatigue on exercise” (JF Mowbray, GE Yousef. BMB 1991:47:4:886-894).
Possible Impairment of PGC-1α causes rapid lactic acid build up in ME / CFS
Summermatter S, Santos G, Pérez-Schindler J, Handschin C (2013) Skeletal muscle PGC-1α controls whole-body lactate homeostasis through estrogen-related receptor α-dependent activation of LDH B and repression of LDH A. Proc Natl Acad Sci U S A 110(21):8738– 43. doi:10.1073/pnas.1212976110
.Bonen A (2009) PGC-1alpha-induced improvements in skeletal muscle metabolism and insulin sensitivity. Appl Physiol Nutr Metab 34(3):307–14. doi:10.1139/H09-008 261.
Leone TC, Lehman JJ, Finck BN, Schaeffer PJ, Wende AR, Boudina S, Courtois M, Wozniak DF, Sambandam N, BernalMizrachi C, Chen Z, Holloszy JO, Medeiros DM, Schmidt RE, Saffitz JE, Abel ED, Semenkovich CF, Kelly DP (2005) PGC- 1alpha deficiency causes multi-system energy metabolic derangements: muscle dysfunction, abnormal weight control and hepatic steatosis. PLoS Biol 3(4):e101
.Handschin C, Spiegelman BM (2008) The role of exercise and PGC1alpha in inflammation and chronic disease. Nature 454(7203):463–9. doi:10.1038/nature07206
Austin S, St-Pierre J (2012) PGC1α and mitochondrial metabolism—emerging concepts and relevance in ageing and neurodegenerative disorders. J Cell Sci 125(Pt 21):4963–71. doi:10.1242/jcs. 113662 268.
“Skeletal samples were obtained by needle biopsy from patients diagnosed clinically as having CFS (and) most patients fulfilled the criteria of the Centres for Disease Control for the diagnosis of CFS (Holmes et al 1988)…These data are the first demonstration of persistence of defective virus in clinical samples from patients with CFS…We are currently investigating the effects of persistence of enteroviral RNA on cellular gene expression leading to muscle dysfunction” (L Cunningham, RJM Lane, LC Archard et al. Journal of General Virology 1990:71:6:1399-1402).
“These results suggest there is persistence of enterovirus infection in some CFS patients and indicate the presence of distinct novel enterovirus sequences…Several studies have shown that a significant proportion of patients complaining of CFS have markers for enterovirus infection….From the data presented here…the CFS sequences may indicate the presence of novel enteroviruses…It is worth noting that the enteroviral sequences obtained from patients without CFS were dissimilar to the sequences obtained from the CFS patients…This may provide corroborating evidence for the presence of a novel type of enterovirus associated with CFS” (DN Galbraith, C Nairn and GB Clements. Journal of General Virology 1995:76:1701-1707).
“We will report at the First International Research Conference on Chronic Fatigue Syndrome to be held at Albany, New York, 2-4 October 1992, our new findings relating particularly to enteroviral infection…We have isolated RNA from patients and probed this with large enterovirus probes…detailed studies...showed that the material was true virus…Furthermore, this virus was shown to be replicating normally at the level of transcription. Sequence analysis of this isolated material showed that it had 80% homology with Coxsackie B viruses and 76% homology with poliomyelitis virus, demonstrating beyond any doubt that the material was enterovirus” (Press Release for the Albany Conference, Professor Peter O Behan, University of Glasgow, October 1992).
“In the CFS study group, 42% of patients were positive for enteroviral sequences by PCR, compared to only 9% of the comparison group…Enteroviral PCR does, however, if positive, provide evidence for circulating viral sequences, and has been used to show that enteroviral specific sequences are present in a significantly greater proportion of CFS patients than other comparison groups” (C Nairn et al. Journal of Medical Virology 1995:46:310-313).
“Samples from 25.9% of the PFS (postviral fatigue syndrome) were positive for the presence of enteroviral RNA, compared with only 1.3% of the controls…We propose that in PFS patients, a mutation affecting control of viral RNA synthesis occurs during the initial phase of active virus infection and allows persistence of replication defective virus which no longer attracts a cellular immune response” (NE Bowles, RJM Lane, L Cunningham and LC Archard. Journal of Medicine 1993:24:2&3:145-180).
“These data support the view that while there may commonly be asyptomatic enterovirus infections of peripheral blood, it is the presence of persistent virus in muscle which is abnormal and this is associated with postviral fatigue syndrome…Evidence derived from epidemiological, serological, immunological, virological, molecular hybridisation and animal experiments suggests that persistent enteroviral infection may be involved in… PFS” (PO Behan et al. CFS: CIBA Foundation Symposium 173, 1993:146-159).
Seeking to detect and characterise enterovirus RNA in skeletal muscle from patients with (ME)CFS and to compare efficiency of muscle metabolism in enterovirus positive and negative (ME)CFS patients, Lane et al obtained quadriceps biopsy samples from 48 patients with (ME)CFS. Muscle biopsy samples from 20.8% of patients were positive, while 100% of the controls were negative for enterovirus sequences. Lane et al concluded: “There is an association between abnormal lactate response to exercise, reflecting impaired muscle energy metabolism, and the presence of enterovirus sequences in muscle in a proportion of (ME)CFS patients” (RJM Lane, LC Archard et al. JNNP 2003:74:1382-1386).
CBT
Twisk F, Maes M: A review on cognitive behavioral therapy (CBT) and graded exercise therapy (GET) in myalgic encephalomyelitis (ME)/chronic fatigue syndrome (CFS): CBT/GET is not only ineffective and not evidence-based, but also potentially harmful for many patients with ME/CFS. Neuro Endocrinol Lett 2009, 30:284-299.
Heins MJ, Knoop H, Prins JB, Stulemeijer M, van der Meer JWM, Bleijenberg G.
Possible detrimental effects of cognitive behaviour therapy for chronic fatigue
syndrome.
Psychother Psychosom
(
2010
)
7
9
:
249
-
256.
Song S, Jason LA: A population-based study of chronic fatigue syndrome (CFS) experienced in differing patient groups: An effort to replicate Vercoulen et al's model of CFS. J Ment Health 2005, 4:277-289.
Roberts AD, Charler ML, Papadopoulos A, Wessely S, Chalder T, Cleare AJ: Does hypocortisolism predict a poor response to cognitive behavioural therapy in chronic fatigue syndrome? Psychol Med 2010, 40:515-522
Jason LA, Torres-Harding S, Brown M, Sorenson M, Donalek J, Corradi K, Maher K, Fletcher MA: Predictors of change following participation in non-pharmacologic interventions for CFS. Tropl Med Health 2008, 36:23-32.
Maes M, Twisk F: Chronic fatigue syndrome: la bête noire of the Belgian Health Care System. Neuro Endocrinol Lett 2009, 30:300-311.
The functional status and well being of people with myalgic encephalomyelitis/chronic fatigue syndrome and their carers. Luis C Nacul, Eliana M Lacerda, Peter Campion, Derek Pheby, Maria de L Drachler, José C Leite, Fiona Poland, Amanda Howe, Shagufta Fayyaz and Mariam Molokhia
LaManca JJ, Sisto SA, DeLuca J, Johnson S, Lange G, Pareja J, et al.
Influence of
exhaustive treadmill
exercise on cognitive functioning in chronic fatigue syndrome.
Am
J Med
(
1998
)
105
: 59S
-
65S. doi: 10.1016/S0002
-
9343(98)00171
-
5.
Suárez A, Guillamo E, Roig T, Blázquez A, Alegre J, Bermúdez J, et al.
Nitric oxide
metabolite production during exercise in chronic fatigue syndrome: a case
-
control
study.
J Womens Health (Larchmt)
(
2010
)
19
:
1073
-
1077.
“The patients with ME/CFS (indicated) profound physical impairment. These scores tended to be below the published norm for patients with cancer, congestive heart failure and myocardial infarction” (J Nerv Ment Dis 2003:191:324-331)
Maes M, Mihaylova I, Kubera M, Bosmans E: Not in the mind but in the cell: increased production of cyclo-oxygenase-2 and inducible NO synthase in chronic fatigue syndrome. Neuro Endocrinol Lett 2007, 28:463-469.
Patrick Neary J, Roberts AD, Leavins N, Harrison MF, Croll JC, Sexsmith JR.
Prefrontal cortex oxygenation during incremental exercise in chronic fatigue syndrome.
Clin Physiol Funct Imaging
(
2008
)
28
:
364
-
372. doi: 10.1
111/j.1475
-
097X.2008.00822.x.
Vermeulen RCW, Kurk RM, Visser FC, Sluiter W, Scholte HR.
Patients with chronic
fatigue syndrome performed worse than controls in a controlled repeated exercise study
despite a normal oxidative phosphorylation capacity.
J Tran
sl Med
(
2010
)
8
:
93. doi:
10.1186/1479
-
5876
-
8
-
93.
VanNess JM, Snell CR, Stevens SR, Bateman L, Keller BA. Using serial
cardiopulmonary exercise tests to support a diagnosis of chronic fatigue syndrome.
Med
Sci Sports Exerc
(
2006
)
38
:
S85. doi: 10.1249/000
05768
-
200605001
-
00386.
Post Exercise Cytokines
Il1-RA, IL-8, MCP-1 (CCL2) were significantly lower in CFS after one CPET. IL1-RA went down more on day 2 for CFS, and up in controls. Strong indication of immune system dysregulation. Plasma Cytokines in ME/CFS Patients and Controls Before and After a Cardiopulmonary Exercise Test. Ludovic Giloteaux, Betsy A. Keller, and Maureen R. Hanson. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
He J, Hollingsworth KG, Newton JL, Blamire AM. Cerebral vascular control is
associated with skeletal muscle pH in chronic fatigue syndrome patients both at rest and
during dynamic stimulat
ion.
Neuroimage Clin
(
2013
)
2
:
168
-
73.
Jammes Y, Steinberg JG, Delliaux S: Chronic fatigue syndrome: acute infection and history of physical activity affect resting levels and response to exercise of plasma oxidant/antioxidant status and heat shock proteins. J Intern Med 2011, 272:74-84.
Jammes Y, Steinberg JG, Mambrini O, Bregeon F, Delliaux S: Chronic fatigue syndrome: assessment of increased oxidative stress and altered muscle excitability in response to incremental exercise. J Intern Med 2005, 257:299-310.
Jammes Y, Steinberg JG, Delliaux S, Brégeon F (2009) Chronic fatigue syndrome combines increased exercise-induced oxidative stress and reduced cytokine and Hsp responses. J Intern Med 266(2):196–206. doi:10.1111/j.1365-2796.2009.02079.x
De Becker P, Roeykens J, Reynders M, McGregor N, de Meirleir K. Exercise capacity
in chronic fatigue syndrome. Arch Intern Med (2000) 160: 3270-3277. doi:
10.1001/archinte.160.21.3270.
Fatigue in adults with post-infectious fatigue syndrome: a qualitative content analysis. Eva Stormorken, Leonard A. Jason and Marit Kirkevold. BMC Nursing 201514:64 DOI: 10.1186/s12912-015-0115-5
Farquhar WB, Hunt BE, Taylor JA, Darling SE, Freeman R. Blood volume and its
relation to peak O(2) consumption and physical activity in patients with chronic fatigue.
Am J Physiol Heart Circ Physiol (2002) 282: H66-H71.
The following have been found in relation to exercise and ME
An oxidative stress study measuring protein carbonyls suggested higher levels of protein oxidation in CFS subjects as opposed to controls.
Exercise testing in 189 CFS subjects resulted in clinically significant subgroups with 50% of subjects showing moderate to severe functional impairment. An unexpected blunting of Heart Rate and Blood Pressure responses was noted.
Sarcoplasmic reticulum defect: conduction and calcium transport abnormalities.
Cardiac muscle—cardiac output found related to illness severity and the predicted exercise-induced relapse.
Subset of CFS patients with IgM-EBV or CMV-Antibody found to be at risk for cardiac motility abnormalities and occasionally true cardiomyopathy.
Raises the issue of incomplete viral replication activating immune responses as suggested by Glaser et al. Sources: Smirnova IV, “Elevated Levels of Protein Carbonyls in Sera of Chronic Fatigue Syndrome patients,” Mol Cell Biochem Jun 248(1-2) (2003): 93-5.
Vanness JM et al, "Subclassifying Chronic Fatigue Syndrome through Exercise Testing." Med Sci Sports Exerc. Jun 35(6) (2003): 908-913. Fulle S et al, “Modification of the Functional Capacity of Sarcoplasmic Reticulum Membranes in Patients Suffering from Chronic Fatigue Syndrome,” Neuromuscular Disorders 13 (2003): 479–484.
Peckerman A et al, "Abnormal Impedance Cardiography Predicts Symptom Severity in Chronic Fatigue Syndrome," Am J Med Sci. Aug 326(2) (2003): 55-60.
Lerner AM et al,"Prevalence of Abnormal Cardiac Wall motion in the Cardiomyopathy Associated with Incomplete Multiplication of Epstein-Barr Virus and/or Cytomegalovirus in Patients with Chronic Fatigue Syndrome," In Vivo 18( 4) (2004): 417-424.
Glaser R et al, “Stress-associated Changes in the Steady-state Expression of Latent Epstein–Barr virus: Implications for Chronic Fatigue Syndrome and Cancer,” Brain Behavior and Immunity 19 (2) (2005): 91-103.
Jones DE, Hollingsworth KG, Jakovljevic DG, Fattakhova G, Pairman J, Blamire AM,
et al. Loss of capacity to recover from acidosis on repeat exercise in chronic fatigue
syndrome: a case-control study. Eur J Clin Invest (2012) 42: 186-194. doi:
10.1111/j.1365-2362.2011.02567.x.
44.
Working Party on CFS/ME (January 2002). "Report of the Working Party on CFS/ME to the Chief Medical Officer for England and Wales". Department of Health
O’Neill CA, Stebbins CL, Bonigut S, Halliwell B, Longhurst JC (1996) Production of hydroxyl radicals in contracting skeletal muscle of cats. J Appl Physiol 81(3):1197–1206
Pattwell DM, McArdle A, Morgan JE, Patridge TA, Jackson MJ (2004) Release of reactive oxygen and nitrogen species from contracting skeletal muscle cells. Free Radic Biol Med 37(7): 1064–1072
Farquhar WB, Hunt BE, Taylor JA, Darling SE, Freeman R (2002), "Blood volume and its relation to peak O2 consumption and physical activity in patients with chronic fatigue", Am J Physiol Heart Circ Physiol, Jan;282(1):H66-71
Fulle S, Pietrangelo T, Mancinelli R, Saggini R, Fano G: Specific correlations between muscle oxidative stress and chronic fatigue syndrome: a working hypothesis. J Muscle Res Cell Motil 2007, 28:355-362.
Abnormal Heat Shock Protein responses during exercise and for a prolonged period thereafter
Thambirajah AA, Sleigh K, Stiver HG, Chow AW. Differential heat shock protein
responses to strenuous standardized exercise in chronic fatigue syndrome patients and
matched healthy controls.
Cli
n Invest Med
(
2008
)
31
:
E319
-
E327.
'Post
viral fatigue syndrome' CRC Critical Reviews in Neurobiology, 4, no.2
[1988]: 157-178
by Professor Peter Behan, The Institute of Neurological Sciences,
University of Glasgow, Scotland.
D.L.
Arnold et al., 'Excessive Intracellular Acidosis of Skeletal Muscle on
Exercise in a patient with a Post-Viral Exhustion Fatigue Syndrome',
Lancet, 1, 8391, [1984]: 1367-1369
General Effects of exercise and stress on ill bodies
Fisher
-
Wellman K, Bloomer RJ. Acute exercise and oxidative stress: a 30 year history.
Dyn Med
(
2009
)
8
:
1. doi: 10.1186/1476
-
5918
-
8
-
1
.
Sakharov DA, Maltseva DV, Riabenko EA, Shkurnikov MU, Northoff H, Tonevitsky
AG, et al. Passing the anaerobic threshold is associated with substantial changes in the
gene expression profile in white blood cells.
Eur J Appl Physiol
(
2012
)
112
:
963
-
972.
do
i: 10.1007/s00421
-
011
-
2048
-
3.
Mogharnas M, Gaeini AA, Sheikholeslami Vatani D, Faraji H. Effects of aerobic and
anaerobic training on inflammatory markers in rats.
Med Sport
(
2011
)
64
:
21
-
30
Millard AL, Valli PV, Stussi G, Mueller NJ, Yung GP, Seebach JD.
Brief exercise
increases peripheral blood NK cell counts without immediate functional changes, but
impairs their responses to ex vivo stimulation.
Front Immunol
(
2013
)
4
:
125. doi:
10.3389/fimmu.2013.00125.
Steensberg A, Toft AD, Bruunsgaard H, Sandmand M
, Halkjaer
-
Kristensen J, Pedersen
BK. Strenuous exercise decreases the percentage of type 1 T cells in the circulation.
J
Appl Physiol
(
2001
)
91
:
1708
-
1712.
Bloomer RJ, Goldfarb AH, Wideman L, McKenzie MJ, Consitt LA. Effects of acute
aerobic and anaerobic
exercise on blood markers of oxidative stress.
J Strength Cond
Res
(
2005
)
19
:
276
-
285.
Lamprecht M, Frauwallner A. Exercise, intestinal barrier dysfunction and probiotic
supplementation.
Med Sport Sci
(
2012
)
59
:
47
-
56.
CBT and GET are treatments for Depression and mental illness. Psychiatry is an inexact and imprecise science. It relies on subjective opinions and views not on medical and scientific facts and evidence. ME is not depression and not mental illness. The following article supported by research findings shows this
Oxidative stress levels are raised in chronic fatigue syndrome and are associated with clinical symptoms. Gwen Kennedy, Vance Spence, Jill Belch et al. Free Radical Biology and Medicine 2005:39:584-589
See section on this web site concerning abnormal red blood
cell structure. (red blood cells are involved in oxygen delivery to
muscles and organs)
"In
'The Psychophysiology of Respiration', Somatics 1993, R. Miller
pointed out one of the things that happens to a Type A is the
breathing pattern changes to something shallow. Carl Reich, MD, has
pointed out the same breathing pattern takes place in asthma and other
diseases involving anxiety and fatigue. Shallow breathing reduces the
oxygen content of the blood. It retains too much, or too little carbon
dioxide. Too much carbon dioxide makes the heart beat faster to
deliver what little oxygen there is to the brain.
Too little oxygen to the cells of the body, and we use the lactic acid
pathway to produce energy just as normal healthy people do after
prolonged exercise, Lehninger, Principles of Organic Chemistry. Molly
Herzschlag, in "CoQ10, Malic Acid, & Magnesium," CFIDS
Chronical summer 1993, explained it as either gluconeogenesis, or
autocannabalism of the muscle tissue brought on by the lack of ATP
from "bioavailable sources." She mentioned also that malic
acid is useful under low oxygen conditions, where "Malic acid
also helps reduce lactic acid build-up in muscles." What is not
all that clear is how that works and why"
Personality may just be the key: the Type A personality breathes too
shallowly. With oxygen poor conditions brought on by shallow breathing
or tension, you put yourself in the same place as an athlete AFTER the
race. Lactic acid build-up is the reason why exercisers experience
pain after an extended workout and why some people get stiff necks
under stress. When lactic acid is injected into normal healthy resting
people, it can create tension, anxiety, fear and panic, smothering and
choking sensations, difficulty in breathing, Drs. Pitts and McClure,
New England Journal of Medicine, Dec. 21, 1967. These symptoms are
experienced by many people with Chronic Fatigue Syndrome and many
people with chronic illnesses of all kinds including Multiple Chemical
Sensitivity. Doctors who believe that such things are "all in the
head" apparently overlooked the biochemistry of lactic acid and
shallow breathing. If you're tense, hurried, or overworked, you're
going to set yourself up for mysterious pains, fatigue, and emotional
disturbances for physical reasons.
Shallow breathing makes the body produce lactic acid to get its
energy. Some consequences are muscle pains and anxiety. One solution
is extra calcium, which binds with lactic acid, neutralizing its
effects by forming calcium lactate, according to Pitts, McClure, and
Reich
http://www.mall-net.com/cooter/oxy.html
Defect
of oxidative metabolism, with resultant acceleration of glycolysis in
muscle tissue. This means that muscle cells are quickly depleted of
ATP and exhaustion is reached more rapidly
Wong R et al, Chest l992; 102: 1716
Behan WMH, Holt J, Kay DH, Moonic P (1999), "In vitro Study of Muscle Aerobic Metabolism in Chronic Fatigue Syndrome", Journal of Chronic Fatigue Syndrome
Myalgic Encephalomyelitis Then and Now. AM Ramsay EG Dowsett. In.. The Clinical and Scientific Basis of Myalgic Encephalomyelitis Chronic Fatigue Syndrome. Ed: BM Hyde, J Goldstein, P Levine. pub: The Nightingale Research Foundation, Ottawa, 1992
From this article:
"The illness, though similar to non-paralytic poliomyelitis in many clinical aspect, could clearly be distinguished and was diagnosed as Benign Myalgic Encephalomyelitis. This name gives a clearer clinical description than many of the eponyms used previously (Iceland Disease, Akureyri's Disease, Epidemic Neuromyasthenia) or invented subsequently (Post viral syndrome, Chronic Fatigue Immune Dysfunction Syndrome). These share the common disadvantage of obscuring the world-wide incidence or of trivializing the clinical severity of the illness."
Short definition of M.E.:
1. Generalised or localised muscle fatigue after minimal with prolonged recovery time.
2. Neurological disturbance, especially of cognitive, autonomic and sensory functions, often accompanied by marked emotional lability and sleep reversal.
3. Variable involvement of cardiac and other bodily systems.
4. An extended relapsing course with a tendency to chronicity.
5. Marked variability of symptoms both within and between episodes.
Stein E (2001), "How to differentiate CFS from Psychiatric Disorder", Presented at The Alison Hunter Memorial Foundation Third International Clinical and Scientific Conference, Sydney, Australia
“The most important thing about exercise is not to have them do aerobic exercise. I believe that even progressive aerobic exercise, especially in phase one and possibly in other phases, is counter-productive. If you have a defect in the mitochondrial function and you push the mitochondria by exercise, you kill the DNA” (Lecture given in Orlando, Florida, February 1999, at the International Congress of Bioenergetic Medicine).
Vermeulen RCW, Kurt RM, Visser FC, Sluiter W, Scholte HR: Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. J Transl Med 2010, 8:93.
Lane RJM, Barrett MC, Woodrow D, Moss J, Fletcher R, Archard LC: Muscle fibre characteristics and lactate responses to exercise in chronic fatigue syndrome. J Neurol Neurosurg Psychiatry 1998, 64:362-367
Arnold DL, Bore PJ, Radda GK, Styles P, Taylor DJ: Excessive intracellular acidosis of skeletal muscle on exercise in a patient with a post-viral exhaustion/fatigue syndrome. Lancet 1984, 1:1367-1369
Wong R, Lopaschuk G, Zhu G, Walker D, Catellier D, Burton D, Teo K, Collins-Nakai R, Montague T: Skeletal muscle metabolism in the chronic fatigue syndrome. In vivo assessment by 31P nuclear magnetic resonance spectroscopy. Chest 1992, 102:1716-1722
In: Chronic Fatigue Syndrome. John Wiley & Sons, Chichester. Ciba Foundation Symposium 173:43-61
LaManca JJ, Sisto SA, DeLuca J, et al. 1998 Influence of exhaustive treadmill exercise on cognitive functioning in chronic fatigue syndrome. Am J Med 105(3A):59S-65S.
ME/CFS patients' ability to work is impaired, as shown by an
abnormal exercise stress test.
They do not recover in 24 hours. Serial testing points to a significant and confirmable physical
abnormality. This test is 100% objective and can prove to the disability companies that ME/CFS
is neither malingering nor faking
From presentations at the 8
th
International Association of Chronic Fatigue Syndrome (IACFS)
Conference, Fort Lauderdale, Florida, held on 10
–
14 January 2007: M Ciccolella and C Snell, Stockton, California
' in those patients whose dynamic or conscientious temperaments urge them to continue effort despite profound malaise or in those who, on the false assumption of 'neurosis', have been exhorted to 'snap out of it' and 'take plenty of excercise' the condition finally results in a state of constant exhaustion. This has been amply borne out by a series of painstaking and meticulous studies carried out by a consultant in physical medicine, himself an ME sufferer for 25 years. These show clearly that recovery of muscle power after exertion is unduly prolonged. After moderate excercise, from which a normal person would recover with nothing more than a good night's rest, an ME patient will require at least 2 to 3 days while after more strenuous excercise the period can be prolonged to 2 or 3 weeks or more. Moreover, if during this recovery phase, there is a further expenditure of energy the effect is cumulative and this is responsible for the unrelieved sense of exhaustion and depression which characterises the chronic case. The greatest degree of muscle weakness is likely to be found in those muscles which are most in use; thus in right- handed persons the muscles of the left hand and arm are found to be stronger than those on the right. Muscle weakness is almost certainly responsible for the delay in accommodation which gives rise to blurred vision and for the characteristic feature of all chronic cases, namely a proneness to drop articles altogether with clumsiness in performing quite simple manoeuvres; the constant dribbling of saliva which is also a feature of chronic cases is due to weakness of the masseter muscles. In some cases, the myalgic element is obvious but in others a careful palpitation of all muscles will often reveal unsuspected minute foci of acute tenderness; these are to be found particularly in the trapezii, gastrocnemii and abdominal rectii muscles.' Source: MYALGIC ENCEPHALOMYELITIS: A Baffling Syndrome With a Tragic Aftermath
By Dr. Melvin Ramsey (1986)
White AT, Light AR, Hughen RW, Bateman L, Martins TB, Hill HR, et al. Severity of symptom flare after moderate exercise is linked to cytokine activity in chronic fatigue syndrome. Psychophysiology 2010; 47: 615-624
Lorna
Paul, physiotherapist, Glasgow Caledonian University. AACFS Conference
Boston 1999.
Clark C, Buchwald D, MacIntyre A, Sharpe M, Wessely S (2002). "Chronic fatigue syndrome: a step towards agreement" (PDF). Lancet 359 (9301): 97–8.
Excessive intracellular acidosis of skeletal muscle on exercise in ME/CFS patients, with a significant abnormality in oxidative muscle metabolism and a resultant acceleration in glycolysis (Proceedings of the Third Annual Meeting of the Society for Magnetic Resonance in Medicine, New York: 1984: 12-13
“In previous studies patients with ME/CFS showed exercise intolerance in incremental exercise tests. We examined venous blood lactate responses to exercise at a work rate below the anaerobic threshold in relation to psychiatric disorder. Our results suggest that some patients with ME/CFS have impaired muscle metabolism that is not readily explained by physical inactivity or psychiatric disorder” (BMJ 1995:311:544-545)
Vanness JM, et al. Subclassifying chronic fatigue syndrome through exercise testing.Med Sci Sports Exerc 2003 Jun;35(6):908-13.
Sorensen B, et al. Complement activation in a model of chronic fatigue syndrome.Allergy Clin Immunol 2003 Aug;112(2):397-403
Elevated
levels of RnaseL are associated with reduced VO2max and exercise
duration in those with CFS. The low tolerance for exercise may be
linked to abnormal oxidative metabolism. The results have implications
for the testing of antiviral therapies in CFS, particularly those
directed at the 2-5A sythease/ribonuclease L pathway.
C. Snell (Philadelphia), AACFS 5th International Research, Clinical
and Patient Conference, 2001
“Exercise Capacity in Chronic Fatigue Syndrome” was unequivocal: “Comparing the exercise capacity in our patients with data from other studies shows a functionality similar to that of individuals with chronic heart failure, patients with chronic obstructive pulmonary disease, and those with skeletal muscle disorder”. Specific findings included (i) the resting heart rate of patients was higher than controls but patients’ maximal heart rate at exhaustion was lower than controls (ii) the maximal workload achieved by patients was almost half that achieved by controls (iii) the maximal oxygen uptake was almost half that achieved by controls. This would affect patients’ physical abilities, leading the authors to comment: “This study clearly shows that patients with ME/CFS are limited in their capabilities”. Taken together, these findings “suggest that alteration in cardiac function is a primary factor associated with the reduction in exercise capacity in ME/CFS” (P De Becker et al. Arch Intern Med 2000:160:3270-3277).
"Wilhelmina
Behan (Glasgow, Scotland) presented an update on current research in
CFS, which she described as characterised by myalgia and exercise
intolerance with unknown pathogenetic mechanisms."
Research paper presented by Wilhelmina Behan (Glasgow, Scotland) to
The Sydney ME / CFS Clinical and Scientific Conference, December 2001
“The data reported here were taken from well-rested subjects andresearch has demonstrated that incremental exercise challenge potentiates a prolonged and accentuated oxidant stress that might well account for post-exercise symptoms in ME/CFS” (J Intern Med 2005: 257 (3):299-310).
Siemionow V, Fang Y, Calabrese L, Sahgal V, Yue GH. Altered central nervous system signal during motor performance in chronic fatigue syndrome. Clin Neurophysiol (2004) 115: 2372-2381. doi: 10.1016/j.clinph.2004.05.012.
Lawrie SM, MacHale SM, Cavanagh JT, O'Carroll RE, Goodwin GM. The difference in patterns of motor and cognitive function in chronic fatigue syndrome and severe depressive illness. Psychol Med (2000) 30: 433-442. doi: 10.1017/S0033291799001816.
Fulcher KY, White PD. Strength and physiological response to exercise in patients with chronic fatigue syndrome. J Neurol Neurosurg Psychiatr (2000) 69: 302-307. doi: 10.1136/jnnp.69.3.302.
Post Exercise effects on cognition and cognitive tasks
Doctors Jay Goldstein and Ismael Mena (USA), using Zenon SPECT brain scans, demonstrated that the physiological brain function of an M.E. patient rapidly deteriorates after exercise. They also demonstrated that this physiological dysfunction could persist for several days following any of several stressors.
VanNess JM, Snell CR, Stevens SR, Stiles TL. Metabolic and neurocognitive responses
to an exercise challenge in chronic fatigue syndrome (CFS).
Med Sci Sports Exerc
(
2007
)
39
:
S445.
Ocon AJ, Messer Z, Medow M, Stewart J. Increasing orthostatic stress impairs
neurocognitive functioning in chronic fatigue syndrome with postural tachycardia
syndrome.
Clin Sci (Lond)
(
2012
)
122
:
227
-
238.
Dickson A, Toft A, O'Carroll RE. Neuropsychological functioning, illness perception, mood and quality of life in chronic fatigue syndrome, autoimmune thyroid disease and healthy participants. Psychol Med (2009) 39: 1567-1576. doi: 10.1017/S0033291708004960.
Constant EL, Adam S, Gillain B, Lambert M, Masquelier E, Seron X. Cognitive deficits in patients with chronic fatigue syndrome compared to those with major depressive disorder and healthy controls. Clin Neurol Neurosurg (2011) 113: 295-302. doi: 10.1016/j.clineuro.2010.12.002.
Caseras X, Mataix-Cols D, Giampietro V, Rimes KA, Brammer M, Zelaya F, Chalder T, Godfrey EL (2006), "Probing the Working Memory System in Chronic Fatigue Syndrome: A Functional Magnetic Resonance Imaging Study Using the n-Back Task", Psychosom Med, Nov-Dec;68(6):947-55.
Tiersky LA, Johnson SK, Lange G, Natelson BH, DeLuca J. Neuropsychology of chronic fatigue syndrome: a critical review. J Clin Exp Neuropsychol (1997) 19: 560-586. doi: 10.1080/01688639708403744.
DeLuca J, Johnson SK, Natelson BH. Information processing efficiency in chronic fatigue syndrome and multiple sclerosis. Arch Neurol (1993) 50: 301-304.
Paul L, Wood L, Behan WM, Maclaren WM. Demonstration of delayed recovery from fatiguing exercise in chronic fatigue syndrome. Eur J Neurol (1999) 6: 63-69. doi: 10.1046/j.1468-1331.1999.610063.x. Task Force for the Diagnosis and Management
Impaired mitochondrial structure and function in ME/CFS patients (JNNP: 2003:74:1382-1386)
In general, following exercise, patients with ME/CFS showed more type I muscle fibre predominance and infrequent muscle fibre atrophy, unlike that which would be expected in healthy sedentary people.(JNNP 1998:64:362-367).
Weinstein AA, Drinkard BM, Diao G, Furst G, Dale JK, Straus SE, et al. Exploratory
analysis of the relationships between aerobic capacity and self
-
reported fatigue in
patients with rheumatoid arthritis, polymyositis, and chronic
fatigue syndrome.
PM R
(
2009
)
1
:
620
-
628. doi: 10.1016/j.pmrj.2009.04.007
Samii A, Wassermann E, Ikoma K, Mercuri B, George MS, O’Fallon A, Dale JK, Straus SE, Hallett M: Decreased postexercise facilitation of motor evoked potentials with chronic fatigue or depression. Neurology 1996, 47:1410-1414.
Samii A, Wassermann EM, Ikoma K, Mercuri B, Hallett M: Characterization of postexercise facilitation and depression of motor evoked potentials to transcranial magnetic stimulation. Neurology 1996, 46:1376-1382.
Hooper PL, Hightower LE, Hooper PL (2012) Loss of stress response as a consequence of viral infection: implications for disease and therapy. Cell Stress Chaperones 17(6):647–55. doi:10.1007/ s12192-012-0352-4
Starr A, Scalise A, Gordon R, Michalewski H, Caramia M: Motor excitability in chronic fatigue syndrome. Clin Neurophysiol 2000, 111:2025-2031.
“Research data gathered around the world enables clinicians to understand, at least in part, musculoskeletal pain in ME/CFS patients…Infection triggers the release of the pro-inflammatory cytokine interleukin-1bwhich is known to play a major role in inducing cyclooxygenase-2 (COX-2) and prostaglandin E2 expression in the central nervous system. Upregulation of COX-2 and prostaglandin E2 sensitises peripheral nerve terminals. Even peripheral infections activate spinal cord glia (both microglia and astrocytes), which in turn enhance the pain response by releasing nitric oxide (NO) and pro-inflammatory cytokines. These communication pathways can explain the wide variety of physiological symptoms seen in ME/CFS. Experimental evidence has shown that ME/CFS patients respond to incremental exercise with a lengthened and accentuated oxidative stress response, explaining muscle pain and post-exertional malaise as typically seen in ME/CFS In many of the published studies, graded exercise therapy has been adopted as a component of the CBT programme (i.e. graded exercise was used as a way to diminish avoidance behaviour towards physical activity). Unfortunately, the studies examining the effectiveness of GET/CBT in ME/CFS did not use musculoskeletal pain as an outcome measure (and) none of the studies applied the current diagnostic criteria for ME/CFS. From a large treatment audit amongst British ME/CFS patients, it was concluded that approximately 50% stated that GET worsened their condition. Finally, graded exercise therapy does not comply with our current understanding of ME/CFS exercise physiology. Evidence is now available showing increased oxidative stress in response to (sub)maximal exercise and subsequent increased fatigue and post-exertional malaise (Manual Therapy 2006:Aug. 11(3):187-189).
Med. Sci. Sports Exerc: 2002:34:1:51-56
They used global transcriptome analysis to identify genes that were differently expressed in the vastus lateralis, and their results are significant. They found that the expression of genes that play key roles in mitochondrial function and oxidative balance (including superoxide dismutase) were altered in ME/CFS patients. Other genes that were altered in these patients include the genes involved in energy production, muscular trophism and fibre phenotype determination.Importantly, the expression of a gene encoding a component of the nicotinic cholinergic receptor binding site was reduced, suggesting impaired neuromuscular transmission. The authors argue that these major biological processes could be involved in and/or responsible for the muscle symptoms of ME/CFS (Int J Immunopathol Pharmacol 2009:22(3):795-807).
Scandinavian Journal of Medicine and Science in Sports 2009: doi:10.1111/j.1600-0838.2009.00895.x
Yoshiuchi K, Cook DB, Natelson BH et al. Physiol Behav July 24, 2007
Doctors Jay Goldstein and Ismael Mena (USA), using Zenon SPECT brain scans, demonstrated that the physiological brain function of an M.E. patient rapidly deteriorates after exercise.
Research
at the Royal Hospital in Adelaide, 1992. Chief researcher Dr Richard
Burnet, speaking in Hobart said when people with CFS use their
muscles, the glucose turns into lactic acid - in effect poisoning
their system. "We believe it is very important, because at long
last it provides some unifying theory that will fit together the
problems these people have," he said.
Schillings ML, Kalkman JS, van der Werf SP, van Engelen BG, Bleijenberg G, Zwartz MJ: Diminished central activation during maximal voluntary contraction in chronic fatigue syndrome. Clin Neurophysiol 2004, 115:2518-2524
Newham DJ, Davies JM, Mayston MJ: Voluntary force generation and activation in the knee muscles of stroke patients with mild spastic hemiparesis. J Physiol 1995, 483:128.
Kent-Braun JA, Miller RG: Central fatigue during isometric exercise in amyotrophic lateral sclerosis. Muscle Nerve 2000, 2000:909-914.
Davey NJ, Puri BK, Nowicky AV, Main J, Zaman R: Voluntary motor function in patients with chronic fatigue syndrome. J Psychosom Res 2001, 50:17-20.
Davey NJ, Puri BK, Catley M, Main J, Nowicky AV, Zaman R: Deficit in motor performance correlates with changed corticospinal excitability in patients with chronic fatigue syndrome. Int J Clin Pract 2003, 57:262-264
Starr A, Scalise A, Gordon R, Michalewski H, Caramia M: Motor excitability in chronic fatigue syndrome. Clin Neurophysiol 2000, 111:2025-2031.
Recent results from a series of MR scans have shown impaired proton removal from muscle during exercise in patients with ME/CFS compared to matched controls. This has led us to hypothesise that fatigue arises due to impaired pH run off from muscle during exercise which is influenced by the degree of autonomic dysfunction”. Professor Julia Newton, ME Research UK International Research Conference held at the University of Cambridge on 6th May 2008
“The use of 31 P-nuclear magnetic resonance (31 P-NMR) has now provided positive evidence of defective oxidative capacity in ME/CFS. Patients with ME/CFS reach exhaustion more rapidly than normal subjects, in keeping with an abnormality in oxidative metabolism and a resultant acceleration of glycolysis in the working skeletal muscles. When the rate of resynthesis of phosphocreatine (PCr) following exercise is measured, this abnormality is confirmed. (This) provides a conclusive demonstration that recovery is significantly delayed in patients with ME/CFS. The results demonstrate that patients with ME/CFS fail to recover properly from fatiguing exercise and that this failure is more pronounced 24 hours after exercise (European Journal of Neurology 1999:6:63-69).
J Nijs, L Paul and K Wallman as a Special Report in J Rehabil Med 2008:40:241-247
The PACE trial The PACE trial in Britain had many deficiencies, flaws and defects which bring its findings into disrepute.
Firstly, they engaged in trial by design by altering the outcome measures at the end of the trial so as to give the impression that an unsuccessful intervention was a success when in fact the results were so bad that several years later, no recovery rates have been published. This is detailed below:
Changes to Recovery markers towards the end of the trial
Original Recovery Criteria
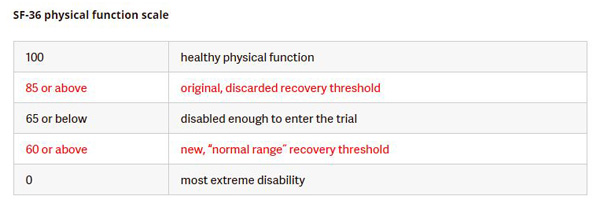
"Recovery" will be defined by meeting all four of the following criteria: (i) a Chalder Fatigue Questionnaire score of 3 or less [27], (ii) SF-36 physical Function score of 85 or above [47, 48], (iii) a CGI score of 1 [45], and (iv) the participant no longer meets Oxford criteria for CFS [2], CDC criteria for CFS [1] or the London criteria for ME [40]. Source:Original PACE Trial Recovery Protocols
(ii) SF-36 physical Function score of 85 or above
This was changed from 85 down to 60.
Their revision of the original outcome measures defining "recovery" makes it look like the researchers could not find any recovered patients using this criteria, so they changed this criteria towards the end of the trial so as to increase the likelihood of finding so called "recoveries". The new recovery marker 60 on the SF-36 scale was lower than the entry level marker to enter the trial 65 on the SF-36 scale , which means some patients, 13%, who entered the trial were already "recovered" according to this criteria before the PACE trial began. This also created the contradiction where a participant could worsen and deteriorate (drop from 65 to 60) and be deemed "recovered" at the end of the trial.
This makes a total nonsense out of their term "recovery", completely undermining the results of the PACE trial. It is considererd unethical, un-scientific and unusual to alter the set or agreed primary outcome criteria of a trial during the trial or at the end of a trial. In addition, this revision of the criteria defining "recovery" contradicts the criteria used in other studies into CBT and GET in ME trials (Bleijenberg et al. BMJ: 2005 January 1; 330: (7481):14). So a person could be very ill with ME and be disabled and they would claim him / her to be "recovered" in the PACE trial, which was a distortion of facts, a ridiculous lie. This alleged 'recovered' state is similar to the average for patients with Class II congestive heart failure.
It is important to be aware that the figure of 60 for "recovery" was used by the Investigators specifically for the
PACE trial and it contradicts how they themselves previously defined markers of recovery in the same disorder
using the same measure: in 2007 they stated: "A patient had to score 80 or higher to be considered as recovered"
(Psychother Psychosom 2007:76:171-176) and in 2009 their Dutch colleagues asserted: "A cut-off of less than or
equal to 65 was considered to reflect severe problems with physical functioning" (European Journal of Public
Health 2009:20:3:251-257).
(i) A Chalder Fatigue Questionnaire score of 3 or less
a Chalder Fatigue Questionnaire score of 3 or less out of maximum 11 to mean recovery was originaly set in the PACE protocol. Patients had to have scored 6 or higher on the 11-point fatigue scale to qualify for the trial and their fatigue could worsen during the trial up to a score of 9 — close to the maximum — and yet they would be classed as within the “normal range” for fatigue. This so called 'normal range' was alleged by he authors to mean recovery. So a person could be very ill with ME and be disabled and they would claim him / her to be "recovered" according to this criteria in the PACE trial, which was a distortion of facts, a ridiculous lie.
Original Recovery criteria: 3 or less (Bimodal scale). Later changed towards the end of the trial to 18 or less (Likert scale) Entry critera: 6 or higher to gain entry (Bimodal scale). Later changed towards the end of the trial to 12 or higher (Likert scale). Using new Likert scale a participant could be improved or recovered before the trial began
This scale was later changed towards the end of the trial from bimodal to Likert. They claimed 18 or less out of maximum of 33 denoted recovery towards the end of the trial - "We therefore considered a score of 18 (highest integral score below the mean plus 1s.D.) or less as within the normal range for fatigue." The figure for 18 or less was far higher than 6 or less which is its direct translation from the original protocol. Yet 12 was the (revised) entry criteria, and an increase to 18 meant worsening of the ilness, so a participant could worsen during the PACE trial and they would claim him / her to be "recovered" using the new criteria. This also created the contradiction where a participant t could be deemed "recovered" according to this criteria before the PACE trial began. A person could be very ill with ME and be disabled and they would claim him / her to be "recovered" in the PACE trial, which was a distortion of facts, a ridiculous lie. This alleged 'recovered' state is similar to the average for patients with Class II congestive heart failure. None achieved the original recovery protocol of 3 or less in the original protocol or 6 or less in the new amended protocol.
(iii) CGI score of 1
This a scale of 1 to 7, with 1 representing recovery and 7 severe illness and disability.
This was changed to 1 or 2 to mean recovery, with 2 representing the 'process of recovery' towards the end of the trial. This inclusion of 2 was not backed up by scientific studies and references. This change or relaxation of the criteria had the objective of finding more so called "recoveries".
(iv) The participant no longer meets Oxford criteria for CFS, CDC criteria for CFS or the London criteria for ME.
' The last protocol requirement for "recovery"—not meeting any of the three case definitions used in the study–was now divided into less and more restrictive sub-categories. Presuming participants met the relaxed fatigue, physical function, and Clinical Global Impression thresholds, those who no longer met the Oxford criteria were now defined as having achieved "trial recovery," even if they still met one of the other two case definitions, the CDC's chronic fatigue syndrome case definition and the ME definition. Those who fulfilled the protocol's stricter criteria of not meeting any of the three case definitions were now defined as having achieved "clinical recovery." The authors did not explain when or why they decided to divide this category into two.
After these multiple relaxations of the protocol definition of “recovery,” the paper reported the full data for the less restrictive category of “trial recovery,” not the more restrictive category of “clinical recovery.” The authors found that the odds of “trial recovery” in the cognitive behavior therapy and graded exercise therapy arms were more than triple those in the adaptive pacing therapy and specialist medical care arms. They did not report having conducted any sensitivity analyses to measure the impact of all the changes in protocol definition of “recovery' '
Source: David Tuller, TRIAL BY ERROR: The Troubling Case of the PACE Chronic Fatigue Syndrome Study
The PACE authors abandoned all of the four criteria specified in the study protocol and replaced them with far weaker ones towards the end of the trial. And they did no sensitivity analysis of the effect of these changes. They provided no detailed explanations and citations to back up these changes. They did not publish the findings from the original protocol and the changed protocol, so that comparisons could be made. This is unscientific and undermines its credibility and validity.
New "recovery" criteria towards the end of the trial
Changing the criteria for recovery or "normal range" from the orignal protocol which used well established and widely used figures (80 - 85 or more on the SF-36 and 3 or less on the Chalder scale) to a new protocol using the mean (average) figure for an ill and disabled patient population was unscientific and unsound, and provides a false recovery or "normal range". Technically (statisically) speaking, they used a non-representative demographic sample to determine recovery thresholds, and inappropriately used a mean and standard deviation for data that doesn’t have a normal distribution, to calculate the normal range. Averaging for sick and ill people while ignoring the original and well established, widely used markers for recovery and improvement, makes a mockery, nonsense and scandal out of this PACE trial and its supporters.
Even 75 or more on SF-36 and 4 or less on Chalder scale would have signalled improvement, but this was not used. These changes were not used for "interpretation purposes" as alleged, but to find new so called "recoveries" or those in the so called "normal range". The PACE researchers should have stuck to the original protocols for recovery and the the 3 limited (non biological) objective markers, and used them at the end, and accepted the findings, whether good or bad.
The World Health Organization (2004), A Practical Guide for Health Researchers states: “Writing the research protocol
“… once a protocol for the study has been developed and approved, and the study has started and progressed, it should be adhered to strictly and should not be changed. This is particularly important in multi-centre studies. Violations of the protocol can discredit the whole study…”
(http://whqlibdoc.who.int/emro/2004/9290213639.pdf)
The Research Councils UK Policy and Code of Conduct on the Governance of Good Research Conduct states:
“All research should be conducted to the highest levels of integrity, including appropriate research design and frameworks, to ensure that findings are robust and defensible. [] This code therefore concentrates on entirely unacceptable types of research conduct. Individuals involved in research must not commit any of the acts of research misconduct specified in this code.”
“Falsification~
This includes the inappropriate manipulation and/or selection of data, imagery and/or consents.”
“Misrepresentation, including: misrepresentation of data, for example suppression of relevant findings and/or data, or knowingly, recklessly or by gross negligence, presenting a flawed interpretation of data;” (http://www.rcuk.ac.uk/documents/reviews/grc/goodresearchconductcode.pdf)
The Medical Research Council (MRC) Guidelines for Good Clinical Practice in Clinical Trials states: “2.5 Clinical trials should be scientifically sound and described in a clear detailed protocol.
2.6 A trial should be conducted in compliance with the protocol that has received prior Ethical Committee favourable opinion.”
(https://www.mrc.ac.uk/documents/pdf/good-clinical-practice-in-clinical-trials/)
They did not subgroup patients according to neurological, endocrine, PEM, infections, illness severity and immune system factors.
The trial had no properly matched control group, and it was unblinded, outcomes or results were subjective not objective. The limited objective tests were unsuccessful in terms of recovery, and were discarded and dismissed as irrelevant at the end of the trial. This is discused in more detail below.
the "English adult population" study they used for the original recovery criteria failed to screen for old age factors, underlying illnesses, diseases and disabilities, physical and intellectual impairments, obesity, total sugar and fat intake, alcoholism, and lifestyle and stress factors in such supposedly "normal" populations. The working age population in good health was not included as the main marker, the criteria. This is a serious error and undermines the reason for revising the primary outcome criteria. And in addition to this error, the bar for "recovery" was then set too low in this trial, and as a result, ill people could be termed "recovered". There has been an accumulation of errors in this trial.+
"Recovery"
In 2016, following several Freedom of Information requests and a court order, the PACE researchers finally releasd the PACE data to the general public. The data showed that recovery as defined in the original published protocol was:
3.1% for specialist medical care alone (SMC)
6.8% for cognitive behavioural therapy (CBT)
4.4% for graded exercise therapy (GET)
1.9% for adaptive pacing therapy (APT)
Source: A preliminary analysis of 'recovery' from chronic fatigue syndrome in the PACE trial using individual participant data. Alem Matthees, Tom Kindlon, Carly Maryhew, Philip Stark, Bruce Levin.21 September 2016 http://www.virology.ws/wp-content/uploads/2016/09/preliminary-analysis.pdf
These figures show that the PACE trial was a failure. In fact the results were less than what one would get from a placebo. In 2013, the PACE researchers had wrongly claimed that CBT led to "recovery" in 22%, GET led to "recovery" in 22%, APT led to "recovery" in 8% and SMC led to "recovery" in 7%. These figures were wrong and over inflated. These figures were also wrong and over inflated. These figures are also discredited by the many flaws and defects in the PACE trial. The improvement itself was subjective, and open to interpretation, and was not supported by objective evidence proposed by the original PACE protocols, and other objective evidence in the form of biological markers. This lack of evidence was worsened by the fact that the markers for "recovery" were changed towards the end of the trial. Furthermore what illness did this tiny number of people recover from ? the diagnostic criteria for the trial was flawed and accepted some people who did not have ME / CFS, but had other illnesses. All of these factors combine together to bring the PACE trial and its findings into disrepute and make them unacceptable in a medical and scientific context.
A 30% recovery rate was cited in the Lancet but was later retracted as it was found to be wrong and misleading.
Half of participants in the standard medical care (SMC) group rated it as not being a logical treatment for them and only 41% were confident about being helped by specialist medical care. (Sharpe, M, Goldsmith, KA, Johnson, AL, Chalder, T, Walker, J, and White, PD. Rehabilitative treatments for chronic fatigue syndrome: long-term follow-up from the PACE trial. Lancet Psychiatry. 2015; 2: 1067–1074).
The standard medical care (SMC) did not involve intensive and comprehensive medical diagnostics and lab tests to identify the biological abnormalities and dysfunctions present and any chronic infections present. Ignoring these biological factors undermined the doctors and the medical treatments given. It was incapable of delivering high quality, accurate treatments. It is no surprise that it's results were similar to CBT and GET, which were disappointing and ineffective. The standard medical care was flawed from a scientific and medical perspective, and cannot be compared or contrasted with any other type of treatment.
The PACE researchers claimed that CBT alone led to improvements in 14% of patients and GET alone led to improvement in 16% of patients. This is a small percentage. They further claimed that 22% "recovered" through CBT and SMC. These figures are discredited by the many flaws and defects in the PACE trial. The improvement itself was subjective, and open to interpretation, and was not supported by objective evidence proposed by the original PACE protocols, and other objective evidence in the form of biological markers. This lack of evidence was worsened by the fact that the markers for "recovery" were changed towards the end of the trial. All of these factors combine together to bring the PACE trial and its findings into disrepute and make them unacceptable in a medical and scientific context.
A 30% recovery rate was cited in the Lancet but was later retracted as it was found to be wrong and misleading.
In 2015, the PACE results show that the overall mean short-form 36 (SF-63) physical functioning score is less than 60. This means most patients are still very ill and disabled. Lupus has a mean score of 63, congestive heart failure has a mean score of 60 while healthy individuals with no illness have a mean score of 93. This means the PACE trial was a failure and that CBT and GET are ineffective. We will also analyse the harms caused by CBT and GET in sections below.
In 2015, the PACE trial follow-up study concluded that outcomes with standard medical care (SMC) alone or adaptive pacing therapy (APT) were similar to CBT and GET at follow-up. (Sharpe, M, Goldsmith, KA, Johnson, AL, Chalder, T, Walker, K, and White, PD. Rehabilitative treatments for chronic fatigue syndrome: long-term follow-up from the PACE trial. Lancet Psychiatry. 2015; 2: 1067–1074)
CBT and GET were no different to receiving no treatment.
the PACE researchers did not state what "recovery" actually meant - did the patients resume full time work ? did they apply for full time work and attend interviews for jobs ? did they go off disability payments and register as being fit for work and available for work with the social welfare and other government departments ? did they feel ready to resume full time work ? were they capable of working 8 - 9 hours a day, 5 days per week ? can they rise early in the morning 7 - 8 am to attend work or training ? was there a return to full health and can this be conclusively proved scientifically and medically ? did they recover the full exercise capabilities of a healthy able bodied person ? did they return to sporting activities ? did they engage in full social activities, dating and relationships, and educational activities of a normal healthy person ?
The PACE researchers have not published details of this in medical and scientific journals.
the missing data in the trial relating to 33 people is ominous and this further undermines it's credibility
will these so called "recoveries" be consistent over 2 - 10 years ? This is important considering the fact that CBT and GET benefits, if any, do not last more than 1 year (8) .
In 2013 and 2015, information on PACE trial details and results were requested by researchers under the Freedom of Information Act in Britain. This request was denied by a tribunal in one case and denied by University authorities in another case, which was very unusual and unexpected. The researchers sought more detailed results including data on patients who deteriorated and worsened after the PACE trial.
Since 2011, PACE authors have tried to block all requests for information about the PACE trial under the Freedom of Information act in Britain. This blocking of data is vexatious to other scientific researchers, medical doctors and patients. And is creating a vexatious relationship between the PACE researchers and other parties. Why yhe blocking and refusals, are the PACE authors covering up ? have they something to hide ? This goes against scientific principles of transparency, openness, opportunities for replication and verification, and integrity and honesty.
The Declaration of Helsinki states: “36. Researchers, authors, sponsors, editors and publishers all have ethical obligations with regard to the publication and dissemination of the results of research. Researchers have a duty to make publicly available the results of their research on human subjects and are accountable for the completeness and accuracy of their reports.”
They did not publish how many patients recovered and worsened according to the original 4 recovery criteria and the 3 objective criteria at the start if the PACE trial. And did not give independent researchers full access to the raw data
They did not publish how many people dropped out of CBT and GET treatments on the PACE trial
They did not publish how many people got worse from CBT and GET treatments on the PACE trial
The PACE trial did not address the
the harm which exercise does to ME patients, and did not acknowledge the existence of Post Exertional Malaise, Systemic Exertion Intolerance Disease (SEID) and Post Exercise Neuo Immune Exhausation (PENE). I refer PACE authors to the research and clinical findings on this at www.me-ireland.com/scientific/16.htm
in ME and CFS, which can be adversely affected by exercise.
"A review involving patients with cancer or chemotherapyinduced fatigue referenced four studies where oxidative stress was held to be the cause of severe fatigue experienced by patients in those studies [99]. Elevated O&NS is also causatively implicated in the development of severe central or “systemic” fatigue [100–103]. A recent review highlighted seven studies where authors cited a significant positive association between oxidative stress and severity of fatigue in patients diagnosed with CFS [5]. Oxidative stress is dramatically elevated in patients with CFS compared to healthy controls during the conduct and aftermath of exercise [104, 105]." Source: The Neuro-Immune Pathophysiology of Central and Peripheral Fatigue in Systemic Immune-Inflammatory and Neuro-Immune Diseases Morris et al. 2015.
The PACE authors did not track the damaging effects of exercise on dysfunctional mitochondria, heart, circulation, muscles, brain and nervous system, immune system, blood vessels and other body systems in ME patients
Some of the PACE researchers and their supporters called ME and CFS imaginary illnesses, "all in the mind", psychological illnesses, psychosomatic, and "non illness" in the past, and ridiculed and insulted such patients ; some facts are presented here at www.ireland.com/bogus.htm . Some may try to deny this, but their past quotations in public and in papers and correpsondence reveal the facts and truth. Should these type of people be carrying out PACE trials or analysing them and supporting them in public ?
The six centers around England participating in the PACE trial applied different methods for assessing safety. This raises questions about lack of standarisation, lack of consistency, and how to interpret the results, and whether the overall claims of “safety” can be taken at face value.
Conflicts of Interest
Some of the PACE trial leaders had undeclared conflicts of interest, including previous work for the private insurance industry where they classified ME as being a psychiatric disorder, requiring CBT and GET, and ME patients were refused disability benefits and refused lab tests. These PACE researchers made large amounts of money from this work in the past, and expected to continue doing so once the PACE trial findings were published. They continue to have strong links with the insurance industry, and they had a vested interest in obtaining a certain outcome in the PACE trial. The patients in the PACE trial were not informed about this. Some further information about these conflicts of interest are provided here.
One PACE researcher had an undeclared conflict of interest in relation to a newsletter shown to PACE participants which endorsed and praised CBT and GET, using the U.K. clinical guidelines committee and 'independent' testimonials from participants in the PACE trial. She served on the U.K. clinical guidelines committee in the past and the PACE research team and was using the newsletter to promote her previous work for the U.K. clinical guidelines committee. The use of the newsletter in the PACE trial had the effect of influencing how patients viewed the PACE treatments offered. No mention was made of adverse outcomes using CBT and GET and the lack of full recoveries and there was no mention of biological abnormalities and of biological diagnostics and treatments. This brought bias and a placebo effect into the PACE trial. The patients in the PACE trial were not informed about this. Trying to influence and manipulate trial participants (patients) in a certain way in a trial which is unblinded and has subjective outcomes and results is a serious breach of Ethics.
The power of suggestion was cynically used by researchers in a Newsletter given to trial participants to downplay harms, deterioration, and a worsening of symptoms, while encouraging feelings of improvement and feeling better. There was a high risk a 'stockholm syndrome' scenario. The lack of objective markers, blinded trials, placebos, and the use of subjective markers and results which can be skewed by the power of suggestion further undermines the validity of the PACE trial.
The PACE authors claimed that CBT and GET were cost effective to society, but how is it cost effective to keep patients sick and ill for years and decades ? It is estimated that ME costs the US economy over $20 billion per year and imposes similar costs on other countries. It imposes a massive financial burden on health systems, social welfare systems, health insurance systems, businesses, economies, individuals, families, and home care. This financial burden is worsened by the fact that CBT and GET are ineffective and useless in treating complex biological illnesses such as ME, and this imposes a continuous cost and serious financial burden to the aforementioned parties. And constitutes a gross neglect of patients.
Letters to the Lancet and CDC authored by medical doctors and researchers
Dr. James C. Coyne, is Professor of Health Psychology at University Medical Center, Groningen, the Netherlands. He is also Visiting Professor, Institute for Health, Health Care Policy & Aging Research, Rutgers, the State University of New Jersey. Dr. Coyne is Emeritus Professor of Psychology in Psychiatry, where he was also Director of Behavioral Oncology, Abramson Cancer Center and Senior Fellow Leonard Davis Institute of Health Economics. .He gave a very informative lecture about the PACE trial in Edinburgh in 2015.
Professor James Coyne also run a Blog about the PACE trial, which raises points of scientific and medical interest
It was stated to patients in the trial that patient data would be kept secure, but this was not followed, and some patient data went missing, and some was stolen. This breaches the rules and ethics of scientific trials. This is also a case of criminal negligence.
they did not state what beneficial effects GET and CBT would have on the chronic viral and pathogen infections, immune system dysfunctions, autoimmunity factors, HPA axis dysfunctions, Neurological dysfunctions and deficits, mitochondria and krebs cycle abnormalities, methylation cycle blocks, post exercise malaise (PEM), orthostatic intolerance and Postural Tachycardia Syndrome, cardiac abnormalities, etc, consistently found in ME patients. The reason being that CBT and GET cannot treat these medical / biological abnormalities in ME patients.
Wessely school psychiatrists have admitted in the past that CBT and GET cannot cure ME and that the alleged " benefits" are temporary (8). Then why did they waste millions of pounds of British taxpayers money on the PACE trial ?
Dr. White who ran the PACE trial previously published a few studies showing increased cytokine abnormalities and inflammation in ME patients after exercise. Yet he did not bother to measure these markers in the PACE trial, and he did not include them in baseline measurements or outcome measurements. He showed a disregard for his own biological findings in the past. This showed a disregard for scientific method, scientific rigour and for patient safety.
The trial did not produce any objective scientific evidence such as changes in biomarkers and biological markers over time to track and verify these so called "improvements" and "recoveries", and deterioration and relapses.
International Petition by ME and CFS patients asking the CDC and HHS in the USA to independently investigate the PACE trial and remove all references to PACE trial, CBT and GET in treatments for ME, CFS or SEID.
Some recent research into CBT, GET and Pacing in Britain in 2015 contradicts the PACE findings. Of patients who received GET, 74 percent said that it had made them worse. While 18 percent said they were worse after cognitive behavior therapy and only 14 percent after pacing.
The PACE trial and results are discredited, meaningless, and useless in a scientific context and medical context. It is also wasteful of government funds and private funds.
Other psychiatrists have claimed that cognitive behavior therapy and exercise therapy had a beneficial effect in their "ME trials" - for whom ? their psychiatric patients or those with diseases other than ME ? Their scientific "trials" had no full recoveries from ME and nobody was able to return to full time work and resume a normal working life and social life and recover the full exercise capabilities of a normal healthy person. Furthermore, they did not test for bio-markers for each of the abnormalities and dysfunctions present in ME and other objective data prior to, during and after these tests, in order to establish progress and recovery, and they did not continue this for 12 months, 24 months, 36 months to measure efficacy, safety and overall effectiveness. And they ignored all the biological and biomedical evidence that exercise can be damaging to ME patients, and ignored the relapses and worsening of symptoms from exercise in ME (6). Furthermore they consistently ignored the scientific and medical evidence that ME is a serious physical biomedical illness as shown by over 5,000 research papers. These trials tend to be sloppy, badly designed, inaccurately recruited, unethical and have far too much psychiatric bias and they should be retracted and rejected by scientific journals.
Evidence that the Wessely School knows that CBT and GET provide no lasting benefit in ME/CFS
Despite their ruthless determination to implement CBT and GET across the board for people with ME/CFS, Wessely School members have previously acknowledged that there is no long-term benefit from CBT, for example:
at the American Association for CFS (AACFS, now the IACFS/ME) International Conference at Cambridge, Massachussets on 10-11th October 1998, Wessely School psychiatrist Michael Sharpe went on record stating that the benefits of CBT faded with time
in a personal communication dated 12th October 1998 to Professor Fred Friedberg, Michael Sharpe stated about his often-quoted 1996 study (BMJ 1996:312:22-26) that outcome measures had begun to decline 17 months after treatment termination (quoted in JCFS 1999:5:3/4:149-159)
on 3rd November 2000, Sharpe again confirmed: “There is a tendency for the difference between those receiving CBT and those receiving the comparison treatment to diminish with time due to a tendency to relapse in the former” ( www.cfs.inform/dk )
the very modest benefit in only some patients who have undergone CBT has been shown to last for only 6-8 months and “observed gains may be transient” (Long-term Outcome of Cognitive Behavioural Therapy Versus Relaxation Therapy for Chronic Fatigue Syndrome: A 5-Year Follow-Up Study. Alicia Deale, Trudie Chalder, Simon Wessely et al. Am J Psychiat 2001:158:2038-2042)
in his Summary of the 6th AACFS International Conference in 2003, Charles Lapp, Associate Clinical Professor, Duke University and Director, Hopkins-Hunter Centre, NC, stated about CBT that Dr Daniel Clauw (who had studied 1,092 patients) found that at 3 months there were modest gains, but at follow-up at 6 and 12 months, those modest gains were lost (this being an example of “evidence-based” medicine)
Wessely himself is on record stating that CBT doesn’t work for all: in his Editorial (JAMA 19th September 2001:286:11) he stated that CBT and GET are only “modestly effective” and that neither is “remotely curative”
Wessely is also on record as stating: “It should be kept in mind that evidence from randomised trials bears no guarantee for treatment success in routine practice. In fact, many CFS patients, in specialised treatment centres and the wider world, do not benefit from these interventions” (The act of diagnosis: pros and cons of labelling chronic fatigue syndrome. Marcus JH Huibers and Simon Wessely. Psychological Medicine 2006:36: (7): 895-900).
It should not be forgotten that after a course of CBT, there is no objective evidence of improvement (only subjective) and that the transient gains may be illusory (Interventions for the Treatment and Management of Chronic Fatigue Syndrome – A Systematic Review. Whiting P, Bagnall A-M et al. JAMA 2001:286:1360-1368).
Videos about Insurance companies which denied disabled people their lawful payments. Some of these have advised governments. Some psychiatrists work as consultants, advisors, or executives for these insurance companies.
5. Carruthers M. Bruce, Jain Kumar Anil, De Meirleir L., Kenny, et. al. Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. 2003.
Carruthers M.,B., van de Sande I M, De Meirleir. L. K, et al. Myalgic encephalomyelitis: International Consensus Criteria. 2011.
6. Links to scientific and medical research papers below
8. Long-term Outcome of Cognitive Behavioural Therapy versus Relaxation Therapy for Chronic Fatigue Syndrome: A 5-Year Follow-Up Study. Alicia Deale, Trudie Chalder, Simon Wessely et al. Am J Psychiat 2001:158:2038-2042
6th AAME International Conference, Presentation by Dr Daniel Clauw. Study of 1,090 ME patients