Why set up an ME Clinic in Ireland ?
3. How Many ? Population Prevalence and Epidemiology Studies 4. The failure of primary care to deal with this illness - the Epidemic of Misdiagnosis 5. The deaths, suicides and terrible suffering endured by sufferers of ME 6. The existence of medical clinics which have successfully treated ME 7. Clinics to treat ME - 2 Different and Opposing Models
1. Irish Economy. The High Economic and Social Costs of the Illness (i) Cost Benefit-Analysis for the Irish Economy Using the American figure of 1% of the population being afflicted with ME, as oultined and referenced below (1), the number of ME patients in Ireland is 45,812 based on a population of 4,581,269 (2). Some ME sufferers have been diagnosed and some have not been diagnosed due to lack of knowledge of the illness and / or poor diagnostic methods and equipment in this state. It is estimated that 50-60% of people with ME have been undiagnosed with the illness and suffer from an illness they are unaware of. As diagnostic tests, equipment and criteria become more accurate and as doctors become more educated about this illness and specialist clinics become operational, and public awareness of the illness increases, there will be an increase in the number of people diagnosed with this illness. The direct health costs and indirect costs in terms of lost productivity, earnings and GDP has not been calculated for Ireland yet. Use of American economic cost figures for Ireland would provide a general guide, as both are advanced western countries, but are not totally accurate due to some differences between the countries. The nearest we can get to an approximation of economic costs for the Irish economy is the results of some research studies in Britain. Ireland and Britain share similar characteristics in terms of health care systems. The following research paper has tried to quantify the economic effects of ME in Britain The total cost to the Irish economy is 1.290 billion euros plus 549 million euros, giving approximately 1.83 billion euros per year. This is a significant loss to the Irish economy. Cost-Benefit Analysis: the cost of building an ME Clinic would be 45 million euros, which would include a modern clinic with several rooms, and advanced diagnostic equipment. Running it would cost a few million euros per year. Diffusion of Costs and Expanding the Return on Investment The clinic will result in savings of tens of millions of euros per year, as more patients improve and recover. And would over time approach the figure of 1.83 billion euros per year in savings. The clinic will also pay for itself in many other ways. Initially, the clinic will involve considerable outlay of funds to acquire state of the art diagnostic equipment and treatment equipment, yet the investment itself will enable the clinic to differentiate itself from other clinics and hospitals in Europe in terms of quality, accuracy, precision and excellence. This will attract more customers (patients) to the clinic and build a reputation which will sustain high customer numbers over time. Furthermore the clinic could share it's facilities and resources for those with other illnesses. Specifically, the equipment in the ME clinic could be made available to the hospital itself and to other nearby hospitals and clinics for those with other neurological illnesses, endocrine and glandular illnesses, autoimmune illnesses, head injuries, internal injuries, and cardiac illnesses subject to designated time usage and demand levels. This would ensure that the equipment is used regularly and there is adequate payback for the intitial capital investment in the equipment, facilities and personnel. The demand for this will grow as population continues to grow, and as a higher percentage of the population ages, and and more and more people become ill or have accidents. All of the above factors would guarantee an excellent return on investment over the long-term. Government funded clinics There is an urgent need for government funded research clinics into ME in all developed countries. This would involve investing in people, people's health and well being, in people's recovery from illness, and in the productivity of people and accompanying social and economic inclusion of disabled people. Hundreds of billions of pounds / dollars have been wasted on bailing out bankers, bondholders, certain business people and financial institutions who were involved in gambling and legal and regulatory violations. It's time now to invest in people, the health and the productivity of the people. Make this part of the EU / US / Canadian / Australian / Chinese / Japanese / Asian economic stimulus packages to bring about economic recovery. Many governments waste hundreds of millions of euros / dollars on wasteful spending, inefficiencies, pet projects which deliver no real, lasting economic and social benefits ; an example of this being The Waste List: 66 Crazy Ways That The U.S. Government Is Wasting Your Hard-Earned Money . Identifying waste and cutting back on waste and using the money which is saved to Invest in the health and well being of the people would deliver lasting economic and social benefits to a nation over the short term and long term. Staff resources The following staff would be employed full-time or part-time OR subcontracted by the clinic OR their services hired on a case-by-case basis from a nearby hospital, clinic or medical practise. - medical doctors who are knowledgeable about ME The support staff: 6 nurses, 1 receptionist, 1 administrator, 1 exercise technician, 2 radiologists to run scanners, 3 laboratory technicians to test samples. Nurses and / or doctors would take samples from ME patients. Clinic opening hours - 9 hours, 6 days per week. Buildings & Equipment Resources Necessary equipment would include
While samples could be taken from patients and sent to specialist private laboratories for:
While the following diagnostic services could be contracted out to nearby hospitals:
Inpatient facilities for severely disabled The location of an ME clinic within the grounds of Merlin Park hospital in Galway city would be strategically important. Merlin Park Hospital typically has 15 - 20 beds free per week. These free beds could be made available to severely ill ME patients. Up to 20% of ME patients are bedridden and are very disabled. Another 20% have moderate to severe mobility impairments. There is abundant space in Merlin Park Hospital grounds for expansion, and it should be possible to build an inpatient facility for the ME clinic to accommodate 60 patients. This inpatient facility could be attached to both the ME clinic and Merlin Park Hospital and avail of hospital personnel and resources. Inpatient stays could be limited to 4 days so as to avail of thorough diagnostic services and accompanying treatment assessments. This 4 day time limit would enable more patients to be admitted over the course of a month, a year, thus ensuring a high throughput over time. The costs of this ME Clinic must be weighed against the cost of 1.83 billion euros per year in Ireland from doing nothing, these costs are increasing as more people are becoming diagnosed with this illness through improvements in diagnosis and a worsening of an illness. And it must also be weighed against the inward revenue to the Irish state and Irish buisnesses from foreign patients attending this ME clinic, amounting to at least 1 billion euros per year. References 2. Central Statistics Office, Ireland. www.cso.ie
There exists a gap in the Irish and European Union market for effective medical ME diagnosis and treatments. Population prevalence is estimated to be 1% of a population (1). This gives the following statistics. This failure of the British government presents
a market opportunity to provide a new type of ME clinic which treats Irish, British, European and international ME patients enabling them to recover. The Irish ME clinic should have sufficient capacity to cater for Irish patients and international patients, with some room for expansion in the future, as it will
attract thousands of patients from Britain and other European
countries. This expansion in the future could be achieved by the building of another ME clinc in another part of the country in order to cope with strong
and sustained domestic and foreign demand. Several
European countries are continuing to neglect ME patients, with the
result that many are suffering, worsening and dying of the illness. Patients are desperate for
effective diagnosis and treatments in Europe, Russia, the Middle East,
and Asia. This will result in increased business for the
Irish clinic and a substantial inflow of foreign revenues for the
clinic and for the Irish government. These foreign revenues will directly benefit the Irish
government and the exchequer. It will also benefit the local economy as
foreign patients and their families stay in local accommodation and spend
money on food, drink, transport and other services. Financial Benefits for the Irish Economy
Lorusso L, Mikhaylova SV, et al. Immunological aspects of chronic fatigue syndrome. Autoimmun Rev 2009; 8: 287-91. Regional distribution of fatiguing illnesses in the United States: a pilot study. Cynthia Bierl, Rosane Nisenbaum, David C Hoaglin, Bonnie Randall, Ann-Britt Jones, Elizabeth R Unger and William C Reeves. Population Health Metrics 2004, 2:1 The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Lin JM, Resch SC, Brimmer DJ, Johnson A, Kennedy S, Burstein N, Simon CJ. Cost Eff Resour Alloc. 2011 Jan 21;9(1):1. (iii) Improving the Accuracy of ME diagnostics and Population Prevalence in Ireland As already mentioned in the American study below, the accuracy of ME numbers could benefit from This could be further enhanced by gathering data on the effectiveness of various medical treatments and complementary treatments, and recovery rates from ME. This would also involve extensive data mining, involving successful medical clinics, hospitals, doctors practises, combined medical and complementary centres, health insurance bodies, medicare and medicaid data, and government health departments.
2. Cost-Benefit Analysis for the British Economy and the American Economy. The High Economic and Social Costs of the Illness In Britain, with a population of 62.3 million in 2011 (10), it is estimated that 623,000 people have ME, based on the 1% finding as outlined and referenced below (11). Some ME sufferers have been diagnosed and some have not been diagnosed due to lack of knowledge of the illness and / or poor diagnostic methods and equipment in this state. It is estimated that 50-60% of people with ME have been undiagnosed with the illness and suffer from an illness they are unaware of. As diagnostic tests, equipment and criteria become more accurate and as doctors become more educated about this illness and specialist clinics become operational, and public awareness of the illness increases, there will be an increase in the number of people diagnosed with this illness. The direct health costs and indirect costs in terms of lost productivity, earnings and GDP has not been calculated for Britain yet. Use of American economic cost figures for Britain would be inaccurate due to major differences in health care structures, health insurance, state involvement in health care, and differences in lost productivity, lost earnings and tax structures. The following research paper has tried to quantify the economic effects of ME in Britain The total cost to the British economy is £14.13 billion plus £6.23 billion, giving approximately £20.36 billion per year. This is a significant loss to the British economy. Cost-Benefit Analysis: the cost of building 4 large ME Clinics in Britain to service 4 major regions of Britain would be £200 million (4 x £50 million) which would include modern and advanced diagnostic equipment, and running it would cost several million pounds per year. Diffusion of Costs and Expanding the Return on Investment The clinics will result in savings of hundreds of millions of pounds per year, as more patients improve and recover. And would over time approach the figure of £20.36 billion per year in savings. The clinics will also pay for themselves in many other ways. Initially, the clinics will involve considerable outlay of funds to acquire state of the art diagnostic equipment and treatment equipment, yet the investment itself will enable the clinic to differentiate itself from other clinics and hospitals in Europe in terms of quality, accuracy, precision and excellence. This will attract more customers (patients) to the clinics and build a reputation which will sustain high customer numbers over time. Furthermore the clinic could share it's facilities and resources for those with other illnesses. Specifically, the equipment in the ME clinic could be made available to a nearby hospital(s) and clinics for those with other neurological illnesses, endocrine and glandular illnesses, autoimmune illnesses, head injuries, internal injuries, and cardiac illnesses subject to designated time usage and demand levels. This would ensure that the equipment is used regularly and there is adequate payback for the intitial capital investment in the equipment, facilities and personnel. The demand for this will grow as population continues to grow, and as a higher percentage of the population ages, and and more and more people become ill or have accidents. All of the above factors would guarantee an excellent return on investment over the long-term. Government funded clinics There is an urgent need for government funded research clinics into ME in all developed countries. This would involve investing in people, people's health and well being, in people's recovery from illness, and in the productivity of people and accompanying social and economic inclusion of disabled people. Hundreds of billions of pounds / dollars have been wasted on bailing out bankers, bondholders, certain business people and financial institutions who were involved in gambling and legal and regulatory violations. It's time now to invest in people, the health and the productivity of the people. Make this part of the EU / US / Canadian / Australian / Chinese / Japanese / Asian economic stimulus packages to bring about economic recovery. Many governments waste hundreds of millions of euros / dollars on wasteful spending, inefficiencies, pet projects which deliver no real, lasting economic and social benefits ; an example of this being The Waste List: 66 Crazy Ways That The U.S. Government Is Wasting Your Hard-Earned Money . Identifying waste and cutting back on waste and using the money which is saved to Invest in the health and well being of the people would deliver lasting economic and social benefits to a nation over the short term and long term. Staff resources The following staff would be employed full-time or part-time OR subcontracted by the clinic OR their services hired on a case-by-case basis from a nearby hospital, clinic or medical practise. - medical doctors who are knowledgeable about ME The support staff: 9 nurses, 2 receptionists (8 hours x 2), 1 administrator, 2 exercise technicians, 4 radiologists to run scanners, 4 laboratory technicians to test samples. Nurses and / or doctors would take samples from ME patients. Clinic opening hours - 16 hours, 6 days per week. Buildings & Equipment Resources
While samples could be taken from patients and sent to specialist private laboratories for:
While the following diagnostic services could be contracted out to nearby hospitals:
Inpatient facilities for severely disabled The location of an ME clinic within the grounds of a major hospital would be strategically important. A major British hospital typically has 30 - 40 beds free per week. These free beds could be made available to severely ill ME patients. Up to 20% of ME patients are bedridden and are very disabled. Another 20% have moderate to severe mobility impairments. There is abundant space in many hospital grounds for expansion, and it should be possible to build an inpatient facility for the ME clinic to accommodate 100 patients. This inpatient facility could be attached to both the ME clinic and the major hospital and avail of hospital personnel and resources. Inpatient stays could be limited to 4 days so as to avail of thorough diagnostic services and accompanying treatment assessments. This 4 day time limit would enable more patients to be admitted over the course of a month, a year, thus ensuring a high throughput over time. The costs of these ME Clinics must be weighed against the cost of £20.36 billion per year in Britain from doing nothing, these costs are increasing as more people are becoming diagnosed with this illness through improvements in diagnosis and a worsening of an illness. And it must also be weighed against the inward revenue to the British state and British buisnesses from foreign patients attending this ME clinic, amounting to at least £ 3 billion per year. As already mentioned in the American study above, the accuracy of ME numbers could benefit from
USA In the context of Federal and state expenditures on health, and financial expenditures by insurance companies, and losses in national productivity and national income (GDP and GNP) it is important to have accurate figures for the number of people suffering from ME. This would help the US government and the CDC and NIH quantify the financial effects of the illness, allocate resources for research and health care, and assess the financial benefits of effective treatments. The most realistic and conservative estimate of the number of Americans afflicted by ME would be 1% as found by several researchers (11). It is estimated that 50-60% of people with ME have been undiagnosed with the illness and suffer from an illness they are unaware of. As diagnostic tests, equipment and criteria become more accurate and as doctors become more educated about this illness and specialist clinics become operational, and public awareness of the illness increases, there will be an increase in the number of people diagnosed with this illness. The 1% figure is likely to be slightly low, and may increase over time as research and diagnostic methods become more comprehensive and accurate. Using population statistics for 2012 (8) this means that 3.16 million Americans have ME. Using the statistics provided by Jason et al. (7) total direct medical costs of this would be $8,675 x 3,160,000 = $27 billion to the US economy. Using statistics suggested by Reynolds et al. the indirect costs in terms of lost productivity, lost earnings and lost GDP would be $20,000 x 3,160,000 = $63 billion. Combining the direct and indirect costs ($27 billion and $63 billion) gives $90 billion in losses for the American economy per year. ME is proving to be an expensive illness for America. This will require urgent action by the US government and it's health institutes (CDC, NIH), research bodies and top universities. Cost-Benefit Analysis: the cost of building 6 large regional ME Clinics in the USA to service 6 major regions ( East (2), Midwest, South, West (2)) would be $420 million (6 x $70 million) which would include modern and advanced diagnostic equipment, and running it would cost several million dollars per year. Diffusion of Costs and Expanding the Return on Investment The clinics will result in savings of billions of dollars per year, as more patients improve and recover. And would over time approach the figure of $90 billion per year in savings. The clinics will also pay for themselves in many other ways. Initially, the clinics will involve considerable outlay of funds to acquire state of the art diagnostic equipment and treatment equipment, yet the investment itself will enable the clinic to differentiate itself from other clinics and hospitals in the Americas and worldwide in terms of quality, accuracy, precision and excellence. This will attract more customers (patients) to the clinics and build a reputation which will sustain high customer numbers over time. Furthermore the clinic could share it's facilities and resources for those with other illnesses. Specifically, the equipment in the ME clinic could be made available to a nearby hospital(s) and clinics for those with other neurological illnesses, endocrine and glandular illnesses, autoimmune illnesses, head injuries, internal injuries, and cardiac illnesses subject to designated time usage and demand levels. This would ensure that the equipment is used regularly and there is adequate payback for the intitial capital investment in the equipment, facilities and personnel. The demand for this will grow as population continues to grow, and as a higher percentage of the population ages, and and more and more people become ill or have accidents. All of the above factors would guarantee an excellent return on investment over the long-term. Government funded clinics There is an urgent need for government funded research clinics into ME in all developed countries. This would involve investing in people, people's health and well being, in people's recovery from illness, and in the productivity of people and accompanying social and economic inclusion of disabled people. Hundreds of billions of pounds / dollars have been wasted on bailing out bankers, bondholders, certain business people and financial institutions who were involved in gambling and legal and regulatory violations. It's time now to invest in people, the health and the productivity of the people. Make this part of the EU / US / Canadian / Australian / Chinese / Japanese / Asian economic stimulus packages to bring about economic recovery. Many governments waste hundreds of millions of euros / dollars on wasteful spending, inefficiencies, pet projects which deliver no real, lasting economic and social benefits ; an example of this being The Waste List: 66 Crazy Ways That The U.S. Government Is Wasting Your Hard-Earned Money . Identifying waste and cutting back on waste and using the money which is saved to Invest in the health and well being of the people would deliver lasting economic and social benefits to a nation over the short term and long term. Staff resources The following staff would be employed full-time or part-time OR subcontracted by the clinic OR their services hired on a case-by-case basis from a nearby hospital, clinic or medical practise. - medical doctors who are knowledgeable about ME If necessary, their services will be sourced in hospitals, clinics and laboratories outside the ME clinic. The support staff: 10 nurses, 2 receptionists (8 hours x 2), 1 administrator, 2 exercise technicians, 3 radiologists to run scanners, 5 laboratory technicians to test samples. Nurses and / or doctors would take samples from ME patients. Clinic opening hours - 16 hours, 6 days per week. Buildings & Equipment Resources
While samples could be taken from patients and sent to specialist private laboratories for:
While the following diagnostic services could be contracted out to nearby hospitals: Sharing of Facilities and Resources for those with other Illnesses Inpatient facilities for severely disabled The location of an ME clinic within the grounds of a major hospital would be strategically important. A major American hospital typically has 30 - 40 beds free per week. These free beds could be made available to severely ill ME patients. Up to 20% of ME patients are bedridden and are very disabled. Another 20% have moderate to severe mobility impairments. There is abundant space in many hospital grounds for expansion, and it should be possible to build an inpatient facility for the ME clinic to accommodate 150 patients. This inpatient facility could be attached to both the ME clinic and the major hospital and avail of hospital personnel and resources. Inpatient stays could be limited to 4 days so as to avail of thorough diagnostic services and accompanying treatment assessments. This 4 day time limit would enable more patients to be admitted over the course of a month, a year, thus ensuring a high throughput over time. The costs of these ME Clinics must be weighed against the cost of $90 billion per year in the USA from doing nothing, these costs are increasing as more people are becoming diagnosed with this illness through improvements in diagnosis and a worsening of an illness. And it must also be weighed against the inward revenue to the US state and US buisnesses from foreign patients attending this ME clinic, amounting to at least $5 billion per year. American Data Gathering As already mentioned above, the accuracy of ME numbers could benefit from This could be further enhanced by gathering data on the effectiveness of various medical treatments and complementary treatments, and recovery rates from ME. This would also involve extensive data mining, involving successful medical clinics, hospitals, doctors practises, combined medical and complementary centres, health insurance bodies, medicare and medicaid data, and government health departments. All of this data would assist the Federal and state governments to plan resource allocations for research projects, prioritise research objectives, measure the effectiveness of research, quantify the effectiveness or ineffectiveness of medical treatments and complementary treatments, invest in the most successful treatments through state investment or state grants to private clinics and hospitals, and quantify progress over time. This is important given the total ineffectiveness and failure of psychiatric-based treatments, and the effectiveness and success of immune system therapies, anti-viral and anti-pathogen therapies, metabolic normalisation and hormone normalisation therapies being applied in leading clinics and hospitals around the world. These new measures would improve the health of the nation, and it's economic, political and social well being in the present and future.
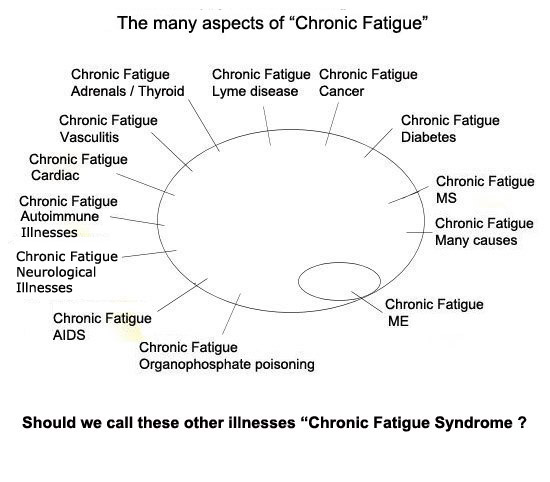
The ME Primer for Healthcare Professionals: based on Myalgic encephalomyelitis: International Consensus Criteria, 2012 puts the figure between 0.4 - 1%. The figure of 1% has been found in several studies below. There are 45,812 ME sufferers in Ireland using the 1% finding from the ME Primer for Healthcare Professionals: based on Myalgic encephalomyelitis: International Consensus Criteria, 2012 and some other international studies. There are 3.16 million Americans afflicted with ME. In Britain, it is estimated that 623,000 people have ME, and 5 million people in the European Union have ME based on the 1% finding (ME Primer for Healthcare Professionals: based on Myalgic encephalomyelitis: International Consensus Criteria, 2012). It is important to note that some ME sufferers have been diagnosed properly using modern and accurate diagnostic criteria and many have not been diagnosed due to lack of knowledge of the illness and / or poor diagnostic methods and equipment in their state / country. It is estimated that 50% or more of people with ME have been undiagnosed with the illness and suffer from an illness they are unaware of. As more modern and accurate diagnostic criteria become accepted by governments and medical authorities, and diagnostic tests and equipment become more advanced and accurate and as doctors become more educated about this illness and specialist clinics become operational, and public awareness of the illness increases, there will be an increase in the number of people diagnosed with this illness. Applying this 1% finding to the global population would suggest that 70,000,000 people have this illness. Though global regional differences may exist due to varying toxic exposures, pathogen exposures, allergen exposures, lifestyle stress factors, pollution of foods, liquids and air, and other illness initiating factors. Population Research Studies There have been no multi-state (25 states or more or 6 distinct regions) studies of ME numbers in the USA, so it is not possible to give an accurate percentage of the total population with ME. Accurate population numbers of ME have not been undertaken by any government and health insurance bodies yet. Though this will change as the health costs and economic costs of this debilitating illnesses continues to increase in a time of limited resources for governments and insurance bodies. Studies by Jason et al. (1) in 1999 suggest that 0.42 % of the US population has ME. This was a limited study with limited feedback from respondents. The population of the US in 2012 was 314,661,000 (8) and 0.42% of this figure is 1.32 million people. However this study conflicts with other studies. Since this study was conducted in 1999, there have been changes to medical and scientific understanding of ME and in diagnostic methodologies.In 2003, research by Bierl et al. (2) stated that 12,186 per 100,000 persons 18 to 69 years of age suffered from fatigue lasting for at least 6 months (chronic fatigue), and 1,197 per 100,000 described an illness that, though lacking clinical evaluation, met criteria for CFS (CFS-like). This suggests that 12% of the American population have Chronic Fatigue and that 1.19% have ME. Using the US population of 2012, this means that 3.8 million people have ME. This is 3 times the number in the 1999 study. Yet this study also lacked precision, as stringent criteria such as the CDC criteria and Canadian Consensus Criteria, and objective diagnostic data for the abnormalities, dysfunctions and infections present in ME were not used. Some people with ME may not have been identified while those who did not have ME may have been included as having ME. However both of these studies conflict with a CDC study by Reyes et al. in 2003 (3) which did a small, limited geographical study in Wichita Kansas. This found a prevalance of 0.235% which is half the number found in the 1999 study by Jason et al. (1) and one sixth the number found by Bierl et al. in 2003 (2). A study of the economic impact of ME by Reynolds et al. (6) used the study of Reyes et al. (3) and their Wichita findings, to propose a figure of 455,000 Americans having ME. This figure of 455,000 people is very low, for example out of a total US population in 2003 of 290,809,777 (8) the figure 455,000 represents 0.156%. This is the lowest figure ever ! And again the lack of precision in identifying genuine ME cases skewed the results of this study. The CDC empirical defintion or Reeves criteria (2005) had several flaws and defects. It was based on the Wichita study which used questionnaires and phone calls. Reeves criteria was very imprecise and inaccurate, and was a sham and had no detailed lab tests, no known biomarkers identification, and no accuate diagnostics such as Canadian criteria (2003), Ramsay criteria, Lake Tahoe criteria to identify genuine ME and CFS cases. They were recruited on the basis of fatigue, a very loose and ambiguous term, which recruited many with other fatiguing illnesses. Reeves himself studied ‘fatiguing illnesses’ not ME and CFS specifically. This muddle created the usual excessive heterogeneity producing confusing, inconsistent and useless findings. The study completely ignored the immune system abnormalities, chronic infections, endocrine abnormalities, brain and neurological abnormalities, brain lesions, neuroinflammation markers, sleep abnormalities, mitochondria abnormalities , inflammatory markers, cardiac and vascular abnormalities. None of these were tested for in the hospital. This research superficially and minimally studied fatigue or fatiguing illnesses, not CFS or ME. Where does great fatigue and exhaustion emerge from ? what causes it ? these questions were never answered via adequate biological tests. Another study by the CDC in 2007 by Reeves et al. (4) conflicts with all of the above studies. It focussed on Georgia in the USA, and on different geographical areas of Georgia and on rural and urban areas, and different exposures and stressors. Interestingly, the study showed a high prevalance of ME in Georgia. It found that 2.54% of the population had ME. This is double the number found by Bierl et al. in 2003, 6 times the number found by Jason et. al in 1999, and 10 times the number found by Reyes et al, in 2003 in Wichita, and 15 times the number proposed by Reynolds et al. (6). If 2.54% of Americans have ME then this means that based on 2012 population statistics (8) that 8 million Americans have ME. This shows yet again, the problem with lack of diagnostic precision in identifying ME cases. An analyis by Jason shows that the Georgia study had several defects and flaws and included people who did not have ME, but other illnesses which were similar, and in some cases had no illness at all. Another study by Jason et al. in 2007 (7) on the economic costs of ME uses the 0.42% finding from a previous study in 1999 by Jason et al. (1). In this paper in 2007, Jason et al. claims that 800,000 Americans have ME, yet 0.42% of a total US population of 281,421,906 for 2000 (the year they used for their study) gives a figure of 1.18 million people. There is a difference between 800,000 and 1.18 million, and the economic costs are signficantly under-stated. Yet, even this figure of 0.42% is small, considerably less than the findings of some other studies. New research in 2013 states a population prevalence of 0.76% (16). This is almost double the 0.4 / 0.42% found in some studies. Another CDC study by Jin et al. (5) in 2011 accepted that 4 million Americans have ME and tried to quantify the health costs (inpatient hospitalizations, provider visits, prescription medication spending, other medical supplies and services) and economic costs (loss in productivity, earnings and income) of ME. The costs were completed for the Georgia economy but not for the US economy. The US population in 2011 was 311,591,917 (8) and a figure of 4 million means that 1.28% of the population have ME. This correlates to the findings of Bierl et al. in 2003 (2) which determined a figure of 1.2%, which amounts to 3.8 million people according to 2012 census figures (8). A Japanese study found a prevalence of 1% (12). This study was limited in size. A Dutch study in 2010 also found a figure of 1% (13). Yet another study found a prevlance ranging from 0.3 - 1% (15). A Dutch study found a prevalence of 3% (17). This figure was very high, and strict criteria such as Canadian criteria and intensive lab tests were not used to identify genuine ME/CFS cases from other illnesses which have fatigue as a symptom. How Many ? (i) Not using strict guidelines and diagnostics to accurately identify ME patients.This would include testing to exclude all other similar illnesses, and then using the International Consensus Criteria (2011) and Canadian Criteria (2003) to diagnose ME cases. The CDC criteria (1994) is outdated and should not be used, as it lacks precision and accuracy. And then verify this criteria through using tests for biomarkers for biological abnormalities, dysfunctions and infections in ME. This then gives a complete descripton of the patient's condition and establishes the ME subgroup a patient belongs to. The prevalence figures in some good studies seem to hover around 1% with a variation +.24 / -.24. Bierl et al. (2), though limited in precision, was a major improvement on other studies, as they focussed on several regions of the USA, and they propose a population prevalance of 1.2%. Again this study had some of the deficiencies as outlined in (i) to (vi) above. Lin et al. (5) in 2011 used the 1.2% figure in their study, amounting to 4 million Americans. This study was an excellent analysis of the economic costs of ME. However, the fact that it was confined to the state of Georgia limits it's applicability at the national level. The Japanese study Hamaguchi et al. (12) found a figure of 1%. . Johnston et al. (16) found a rate of 0.76%. Bates et al. (15) found a prevalence ranging from 0.3 - 1%. The 1% figure is the best approximation based on what limited studies have been done and the fact that diagnosis has been undermined by lack of use of Canadian Consensus and International Cosensus Criteria, high-tech diagnostic equipment, methodologies and tests, and poor medical understanding of the illness (11). We have used the 1% figure to assess population prevalence and the costs of the illness, and the benefits of a clinic and effective treatments (11). The larger problem of chronic fatigue from un-diagnosed illnesses such as Diabetes, Cancer, adrenal disease, thyroid disease, Lyme disease, Vasculitis, parastical infections, Depression, mental illnesses, cardiac abnormalities, MS, AIDS, nutritional deficiencies (also in developed countries), heavy metal toxicity, organophosphate poisoning etc. which cause great fatigue and weakness remains a problem in many countries. Bierl et al. (1) found that 12% of the American population suffer from chronic fatigue which may be caused by one of these aforementioned illnesses, while 1.2% suffer from ME. The great problem is that many are un-diagnosed and many people suffer unnecessarily. Doctor surveys consistently show that over 50% of patients complain of great fatigue while attending their doctor. The diagram below presents this problem of chronic fatigue as it exists in many societies. ME is one of many physical, biomedical illnesses which involve great fatigue or "chronic fatigue". The term "chronic fatigue" is far too general, and too easily open to misinpretation and mis-diagnosis. It is important to differentiate which illness the patient suffers from.
References1. A community-based study of chronic fatigue syndrome.Jason LA, Richman JA, Rademaker AW, Jordan KM, Plioplys AV, Taylor RR, McCready W, Huang CF, Plioplys S. Arch Intern Med. 1999 Oct 11;159(18):2129-37. 2. Regional distribution of fatiguing illnesses in the United States: a pilot study. Cynthia Bierl, Rosane Nisenbaum, David C Hoaglin, Bonnie Randall, Ann-Britt Jones, Elizabeth R Unger and William C Reeves. Population Health Metrics 2004, 2:1 3. Prevalence and incidence of chronic fatigue syndrome in Wichita, Kansas. Reyes M, Nisenbaum R, Hoaglin DC, Unger ER, Emmons C, Randall B, Stewart JA, Abbey S, Jones JF, Gantz N, Minden S, Reeves WC. Arch Intern Med. 2003 Jul 14;163(13):1530-6. 4. Prevalence of chronic fatigue syndrome in metropolitan, urban, and rural Georgia. Reeves WC, Jones JF, Maloney E, Heim C, Hoaglin DC, Boneva RS, Morrissey M, Devlin R. Popul Health Metr. 2007 Jun 8;5:5. 5. The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Lin JM, Resch SC, Brimmer DJ, Johnson A, Kennedy S, Burstein N, Simon CJ. Cost Eff Resour Alloc. 2011 Jan 21;9(1):1. 6. The economic impact of chronic fatigue syndrome. Kenneth J Reynolds, Suzanne D Vernon, Ellen Bouchery and William C Reeves. Cost Effectiveness and Resource Allocation 2004, 2:4 7. The Economic impact of ME: Individual and societal costs. Leonard A Jason, Mary C Benton, Lisa Valentine, Abra Johnson, and Susan Torres-Harding. Dynamic Medicine 2008, 7:6. 8. U.S. Bureau of the Census. Web: www.census.gov. 9. Central Statistics Office, Ireland. www.cso.ie 10. Office for National Statistics http://www.ons.gov.uk/ons/index.html Lorusso L, Mikhaylova SV, et al. Immunological aspects of chronic fatigue syndrome. Autoimmun Rev 2009; 8: 287-91. Regional distribution of fatiguing illnesses in the United States: a pilot study. Cynthia Bierl, Rosane Nisenbaum, David C Hoaglin, Bonnie Randall, Ann-Britt Jones, Elizabeth R Unger and William C Reeves. Population Health Metrics 2004, 2:1 The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Lin JM, Resch SC, Brimmer DJ, Johnson A, Kennedy S, Burstein N, Simon CJ. Cost Eff Resour Alloc. 2011 Jan 21;9(1):1. 12. Hamaguchi M , Kawahito Y , Takeda N , Kato T , Kojima T . Characteristics of chronic fatigue syndrome in a Japanese community population : Chronic fatigue syndrome in Japan. Clin Rheumatol. 2011 Feb 8. PMID: 21302125 13. van't Leven M , Zielhuis GA , van der Meer JW , Verbeek AL , Bleijenberg G . Fatigue and chronic fatigue syndrome-like complaints in the general population. Eur J Public Health. 2010 Jun;20(3):251-7. PMID: 19689970 15. Bates DW , Schmitt W , Buchwald D , Ware NC , Lee J , Thoyer E , Kornish RJ , Komaroff AL . Prevalence of fatigue and chronic fatigue syndrome in a primary care practice. Arch Intern Med. 1993 Dec 27;153(24):2759-65. PMID: 8257251 16. Johnston S , Brenu EW , Staines D , Marshall-Gradisnik S . The prevalence of chronic fatigue syndrome/ myalgic encephalomyelitis: a meta-analysis. Clin Epidemiol. 2013;5:105-10. PMID: 23576883 17. Huibers MJ , Kant IJ , Swaen GM , Kasl SV . Prevalence of chronic fatigue syndrome-like caseness in the working population: results from the Maastricht cohort study. Occup Environ Med. 2004 May;61(5):464-6. PMID: 15090670
Primary care doctors lack the basic knowledge about ME to analyse symptoms, diagnose or treat the illness. Medical schools did not have courses on this illness up until very recently - 2005. So most primary care doctors know very little or nothing about this illness. ME is often wrongly categorised as a psychiatric illness, when it is not. Scientific and medical findings conistently show ME to be a physical illness, comparable in severity to MS, Cancer and AIDS. Doctors lack awareness of the special diagnostic tests and diagnostic markers necessary to make an accurate diagnosis of ME and the abnormalities and dysfunctions present in a patient. They do not know what to look for. This lack of diagnostic information in turn leaves the doctor with no treatment options for the patient. This is further worsened by the fact that the Irish Medical Council has no approved medicines to treat ME. All of these factors have left many patients in a medical limbo, and not able to make any progress. Furthermore, most primary care doctors are very busy, over-worked and under a lot of stress, as a result of increased prevalence of illness in the general population, and they do not have the time to listen to ME patients. Many doctors are forced to give ten minutes or less to each patient. This is not enough time to get an understanding of an ME patient and the complexity of his / her condition. Most ME patients in Ireland and Northern Ireland either remain very ill or get worse over time. Primary care has failed and will continue to fail ME patients. There is an increasing risk of suicide, heart attack and certain Cancers among ME patients in Ireland and several other countries which is laregly linked to this medical limbo and lack of hope - Patient deaths from ME. The only solution is (i) a ME clinic in Ireland with specialists and consultants who have expertise in the area (ii) the legalisation of certain medical drugs to treat ME and their medical designation for ME treatment (iii) the legalisation of certain herbs and supplements to treat ME and their legal designation for ME treatment.
5. The deaths, suicides and terrible suffering endured by sufferers of ME It's important to realise that many people are enduring terrible suffering and many are dying of the health complications caused by ME ( See Memorial section ) . In Ireland thousands of patients are bedridden or confined to wheelchairs or are housebound. A significant percentage rely on home help by social services or by family and friends. ME bears a resemblance to Cancer and AIDS in the sense that many ME patients have died of opportunistic infections due to a depleted immune system. Research also shows that ME patients have serious heart and vascular abnormalities arising from ME, making them highly susceptible to a sudden heart attack. New research shows that ME patients have immune system abnormalities which put them at a high risk of getting certain types of Cancer. There is also a high rate of suicide among ME patients, this being brought about by frustration, desperation for some cure, social isolation, lack of support, constant pain, exhaustion and weakness, and financial hardships. This is being confirmed by research - Patient deaths from ME and Why myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) may kill you: disorders in the inflammatory and oxidative and nitrosative stress (IO&NS) pathways may explain cardiovascular disorders in ME/CFS. On May 12 1995, testifying before a US Congressional briefing, AIDS specialist Mark Loveless told legislators that a ME patient "feels every day significantly the same as an AIDS patient feels two months before death". Mr. Loveless supported his statement with data from research conducted at his own institution and morididity data provided by other ME experts who had compared the two diseases (AIDS and ME). The following passage from the book 'Osler's Web' by Hillary Johnson depicts the devastating effect of ME on people
Source: 'Osler's Web' by Hillary Johnson. Backinprint.com. 2006. Chapter: Gray Hats. Page 674. People are dying of ME and waiting around is not an option. Patients cannot wait another 20, 30, 40, 50 years for the "miracle cure", the "miracle drug", the so called "big breakthrough" in research which will deliver them from their suffering. Most western governments have not financed ME research over the last 30 years, since it first emerged as a public health threat, and they are still not financing ME research. There is a tendency for ME patients to sit around waiting for the "miracle cure", but this is deluded thinking. We have the ridiculous situation of seriously ill ME patients being asked to fund research when they themselves are on the poverty line, receiving small disability payments, and recently experiencing cutbacks in these small disability payments. And they have to pay for high costs of living - in most developed countries, bills are high, rents are high, house prices are high, mortgages are expensive, food prices are high, socialising costs are high, energy costs are high and rising, inflation in basic goods is high, transport costs are high, etc. etc. Scientific studies now show that consumers are being ripped off in some European Union countries, including Ireland. We live in societies where the financially strong extract the maximum amount they can from everybody, including the ill, the sick, the poor, the unemployed, the low paid, and the elderly ; a fact borne out in the taxpayer bail-outs of banks, bank investors and bank bondholders, costing trillions of euros in Europe, the USA and Asia. Since the year 2000, the Federal Reserve in the USA has created $26 trillion in new money to bail out banks and financial institutions from the USA and foreign countries. There is no shortage of money, despite all the claims of such in many countries. ME patients are under a lot of financial pressure today. Most ME patients live in dire poverty and debt, and they just cannot afford to pump money into ME research, which is being under-funded or not funded by governments. We can take action today - there are cases of doctors who have successfully treated thousands of ME patients around the world - what can we learn from them ? We can apply their knowledge, their expertise, their experience in a Clinic specifically devoted to diagnosing and treating ME. A clinic which would be an international centre of excellence. The case for an ME Clinic is clear-cut and straightforward - a diabetic goes to see an endocrinologist in a diabetes clinic a few times a year, someone with Cancer goes to see a Cancer specialist a few times a month, someone with heart disease goes in to see a Cardiologist a few times a year, some with rheumatism goes to see a Rheumatologist a few times a year, someone with Parkinson's disease goes to see a neurologist a few times a year, someone with lupus goes to see their dermatologist and neurologist once a year. Then they have the local doctor to follow up on this and keep it going. So there are two types of doctor assisting a patient - a specialist in a special clinic attached or affiliated to a major hospital and a local doctor in a doctor's practise. In Ireland and Britain, ME patients have no ME specialists and no ME clinics. All they have is a local doctor or GP. The GP or family doctor is incapable of treating and curing ME. There was no mention of ME in medical textbooks and medical training in Ireland until 2005. The average doctor or GP knows very little or nothing about ME, and the vast majority of them are incapable of diagnosing or treating ME. Yet this is all that is available for ME patients in Ireland and Britain at the moment. To worsen this situation, both Ireland does not have the high-tech testing equipment to detect the abnormalities and dysfunctions found in ME. This lack of knowledge and expertise and lack of proper testing and testing equipment means the majority of ME patients are not getting the medical treatment they require. The NICE clinics in Britain are using treatments for psychiatric illnesses to treat ME, which is wrong, misguided and is not succeeding. Treatments such as CBT, GET and psychiatric drugs cannot bring about recovery from ME and are a waste of British taxpayers money. There have been no reports of full recoveries of ME patients in such psychiatric clinics (NICE clinics). In fact there are many reports of ME patients remaining ill or becoming worse after visits to such clinics. This is due to the fact that ME involves several biological abnormalities and dysfunctions and chronic infections, and these cannot be effectively treated with psychiatric treatments. The following testimony by Professor Malcolm Hooper to the British House of Commons in 2007 shows the failure of NICE clinics in Britain - Evidence submitted by Professor Malcolm Hooper The sad fact is that many British ME patients are suffering pain, hardship, and dying of ME because the British government is being poorly advised by psychiatrists and as a result does not have proper ME clinics to treat them. The following video shows a British woman who had ME and was given a bogus psychiatric diagnosis and psychiatric treatments by British doctors. These psychiatric treatments included CBT and exercise therapy. She died. A post-mortem revealed that she had a virus infection of the spinal cord and nervous system and a lot of inflammation of the spinal cord. Psychiatric treatments could not treat this, but some British doctors insisted on psychiatric treatment which led to her death. Click on videos below to watch them.
The Hippocratic oath taken by medical doctors states that a doctor should do no harm. Improper diagnosis and treatments and neglect of this woman through the wrong use of psychiatric medicine meant that serious harm was done to this woman. And, unfortunately many other ME patients are suffering similarly.
6. The existence of medical clinics which have successfully treated ME The top ME clinics in the world below are focussed on diagnosing and treating the biomedical, biological and physical disease processes in ME. Their treatments often include multi-treatments or several treatments at the same time to treat diagnosed medical abnormalities and dysfunctions and infections. North America and South America
Europe
Australasia, Asia and Africa
7. Clinics to treat ME and CFS - 2 Different and Opposing Models
8. The fact that bogus alternative health clinics and alternative medicine
practitioners in Ireland are charging exorbitant fees to patients for useless
treatments which are endangering the lives of such patients
References 1. Campaign for an Irish ME Clinic (web site). Diagnosis and Treatments section, Recovery Database Section, http://www.cfs-ireland.com . Accessed November 2012 2. Sophia and M.E. (web site). 'Psychiatrists paid by outside interests'. http://www.sophiaandme.org.uk/collusion.html Accessed November 2012. Corporate Collusion in denial of treatments THE MENTAL HEALTH MOVEMENT: PERSECUTION OF PATIENTS ? Response by Professor Malcolm Hooper to Wessely receiving the John Maddox Award Videos about Insurance companies which denied disabled people their lawful payments. Some of these have advised governments. Some psychiatrists work as consultants, advisors, or executives for these insurance companies.
3. Myalgic encephalomyelitis: International Consensus Criteria, 2011.This supercedes 'Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols (2003)' listed below. 4. Jason LA, Najar N, Porter N, Reh C. Evaluating the Centers for Disease Control’s empirical chronic fatigue syndrome case definition. J Disabil Pol Studies 2009; 20: 91-100. doi:10.1177/1044207308325995 Accessed on 10/02/2011 5. Carruthers M. Bruce, Jain Kumar Anil, De Meirleir L., Kenny, et. al. Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. 2003. 6. Links to scientific and medical research papers below Effects of Exercise, GET and CBT Severely Damaged Mitochondria and Defective Krebs cycle and ATP production Cardiac and Vascular and Blood vessel problems. Increased risk of heart attack 7.Professor Malcom Hooper's Reply to MRC rejection of PACE Trial complaint Response by Professor Malcolm Hooper to Wessely receiving the John Maddox Award Testimony by Professor Malcolm Hooper to the British House of Commons in 2007 8. Long-term Outcome of Cognitive Behavioural Therapy versus Relaxation Therapy for Chronic Fatigue Syndrome: A 5-Year Follow-Up Study. Alicia Deale, Trudie Chalder, Simon Wessely et al. Am J Psychiat 2001:158:2038-2042 6th AAME International Conference, Presentation by Dr Daniel Clauw. Study of 1,090 ME patients Corporate Collusion in denial of treatments See section Effects of Exercise for research listings Medisch Contact, February 2008, ISBN: 978-90-812658-1-2, by Koolhaas MP, de Boorder H, van Hoof E. The Netherlands |