Most medical students and medical schools do not cover the subject of ME. Many doctors do not know about ME and the immune dysfunctions, infections, neurological dysfunctions, endocrine dysfunctions and mitocondria abnormalities in ME. Some doctors wrongly believe it to be a psychological illness. Most doctors do not know about or have not read the best international practises for diagnosing and treating ME, this being Myalgic encephalomyelitis: International Consensus Criteria, 2011 and Myalgic Encephalomyelitis / Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols (2003) . In this section we will provide multimedia presentations about ME, the diagnostics, the treatments, the scientific findings, the clinical findings, the lectures of eminent medical doctors, special courses in Universities and hospitals, and other material to help inform medical doctors about ME
1. Dr. Anthony Komaroff, Professor of Medicine at Harvard Medical School in the USA.He has been treating ME patients and researching the illness since 1987. He is an internationally recognised ME expert. He has advised several Federal Bodies in the USA on the subject of ME over the years.
. 2. Medical Experiences of Dr. John Richardson, a British medical doctor, who treated ME patients for 40 years and researched the illness
Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME.
3. Medical Diagnostic Protocols and Treatment Protocols using Best International Practices
ME is a chronic physical illness, which is multi-factorial, involving immune system dysfunctions, neurological dysfunctions and abnormalities, chronic infections of the nervous system, brain, muscles, glands and intestines in subgroups of patients, HPA axis and endocrine dysfunctions, mitochondria abnormalities and dysfunctions and cardiac and vascular system abnormalities. Chronic Fatigue Syndrome or CFS is a term invented in 1988 and is a false diagnosis. It diagnoses nothing and explains nothing and is useless. Many doctors no longer use the term 'CFS' or 'Chronic Fatigue Syndrome'. This is explained on the home page of this web site. Some doctors and scientific researchers cite previous names for ME such as ‘Epidemic Neuromyasthenia’, 'Atypical Poliomyelitis’, 'Iceland disease', ‘Encephalitis’, 'Encephalitis lethargica', ‘Akureyri Disease’, ‘Poliomyelitis-like epidemic neuromyasthenia’, 'Diencephalitis', ‘Abortive Poliomyelitis’. Fibromyalgia is common in both ME and Chronic Lyme disease patients, and has it's own biological markers. There is international agreement between experienced doctors, scientific researchers, medical authorities and governments in relation to what constitutes ME.
4. Medical Textbooks and Scientific Textbooks and References for doctors, consultants, nurses and medical students
Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME.
Gulf War Syndrome and other illnesses have been researched by Dr. Garth Nicolson and other scientists. Dr. Nicolson has publications, reports and made sworn testimonies to Presidential Commissions and committees of the U. S. Congress. He exposed illegal experiments on US military personnel, exposures to dangerous toxins and tests on people in American nursing homes, prisons and hospitals. http://www.projectdaylily.com
5. Internships in the most successful ME medical clinics in the world. Learning from highly experienced medical doctors with expertise in ME
Medical students, junior doctors and senior doctors / consultants can apply for internships in top ME clinics and learn from the experts in ME. This would greatly enhance one's medical skills and knowledge and allow one to return to one's country or state and effectively treat ME patients and Fibromyalgia patients there. There is a massive and growing demand for such doctors globally.
North America & South America
Dr. John Chia is a medical doctor with expertise in treating ME and CFS. He is Assistant Professor at the UCLA School of Medicine and President of EV Med Research, Director of the Enterovirus Foundation and is an international expert on Enteroviruses and their role in ME and CFS, and other diseases. His work is well acknowledged in North America and Europe.
Address: 23560 Crenshaw Blvd #101, Torrance, CA 90505, United States
of America.
Phone:+1 310-784-5880
The Cheney Clinic in the USA . Dr. Paul Cheney has been treating ME and CFS since 1985. He was one of the doctors involved in treating patients in the Lake Tahoe outbreak in the mid 1980's in the USA. He is a highly regarded medical doctor and researcher, and is one of the most knowledgable doctors on ME and CFS in the world.
Dr. Daniel Peterson, is a well known ME and CFS doctor and researcher. He has been treating the illness since 1985, including treating victims of the Lake Tahoe outbreak in the 1980's. He has a very comprehensive knowledge of the illness. He currently works in Sierra Internal Medicine Associates 926 Incline Way, Incline Village NV 89452. Tel: (775) 832-0989
Dr. Byron Hyde has been involved in ME treatment and research since the mid 1980's and is one of the most experienced ME doctors in the world. Address: Dr. Byron Hyde, Nightingale Research Foundation, 121 Iona Street, Ottawa, Ontario, Canada. Book an Interview with Dr Byron Hyde on Skype or iChat Video
Dr. Alison Bested, in Toronto, Ontario. She is a highly experienced doctor who has been treating ME and CFS since the late 1990's. She was one of the authors of the Canadian criteria (2003).
Dr. Lucinda Bateman's medical clinic in Utah, USA. Dr. Bateman is a highly respected and well experienced medical doctor who has been treating ME patients since the late 1990's. Her expertise in ME has been ackowledged by the US government authorities and national patient organistions in the USA, who have asked her to serve on their committees and bodies.
Dr. Sarah Myhill's Clinic in Britain. Dr. Sarah Myhill is a distinguished and highly regarded medical doctor and researcher based in Wales. Dr. Myhill has been treating ME patients and researching the illness since the mid 1990's.
Dr Hugh Derham
Bicton - Healthquest - Point Walter Medical Centre
322-324 Canning Highway (Cnr Point Walter Rd) Bicton WA 6157. Phone: 08 9438 2299
Bicton - Bicton Medical Centre
National Centre for Neuroimmunology and Emerging Diseases The top ME research facility in Australia. It collaborates with other research institutes around the world in ME research. It has plans to open an ME clinic for patients.
Ehlers-Danlos Syndrome (EDS), commonly found in ME and CFS patients
- The Royal Melbourne hospital familial cancer Centre, affiliated with Melbourne University has a genetics section dedicated to connective tissue diseases including EDS.
- Royal Childrens Hospital - Professor Ravi Savirayan and Mr Gary Nattrass - recommendation from EDS Australia group
- Monash Children's Hospital - Professor Sue Piper - recommendation from EDS Australia group
POTS commonly found in ME and CFS patients.
-
The clinical pharmacology department at the Austin Hospital which is affiliated with Melbourne University includes Specialist POTS Diagnosis and treatment.
Dr. Rosamund Vallings, New Zealand. A medical doctor with over 15 years experience treating ME patients and researching the illness, and one of the authors of the Canadian Criteria (2003) and International Consensus Criteria (2011)
Lymphatic Drainage - identify good practitioners in your country
-
The Perrin Technique: Dr. Raymond Perrin, Britain
6. Doctor Training ProgramsOnline
Dr. Byron Hyde is a medical doctor based in Canada. He has been treating ME patients and researching the illness since 1985. He has seen thousands of ME patients. Dr. Hyde is an internationally recognised ME expert and has contributed much to research, and clinical practise methodologies, including the Canadian Consensus Criteria 2003 and International Consensus Criteria 2011.
Dr. Dan Peterson, is a medical doctor who has been treating ME patients since the mid 1980's and is an internationally acclaimed ME doctor and expert. He was involved in the Lake Tahoe epidemic in the USA in the mid 1980's, and treated many patients and provided samples to the CDC and other Federal bodies. He worked in general practise for many yerars, and at the Whittemore Peterson Institute for several years, and now runs the Sierra Internal Medicine clinic in Nevada. He also serves on Simmaron Research's Scientific Advisory Board. He has seen thousands of ME patients over the years. Lecture by Dr. Dan Peterson below providing a medical and scientific overview of ME (Stockholm, November 2011). 4 continuous videos of his lecture below
Dr. Paul Cheney is a medical doctor and an internationally respected ME expert. He has successfully treated hundreds of ME patients in the USA since the mid 1980's.He was involved in the Lake Tahoe epidemic in the USA in the mid 1980's, and treated many patients and provided samples to the CDC and other Federal bodies. He runs The Cheney Clinic in the USA.
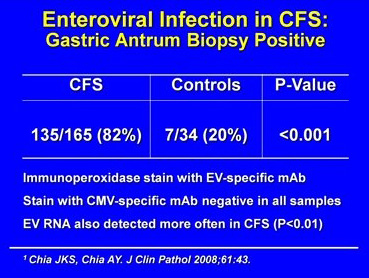
Dr. John Chia, is medical doctor based in California, who is world renowned for his work, particuarly with Enteroviruses. He has been treating ME pateints and researching the illness since the late 1990's. He has found that Enteroviruses are present in some subgroups of ME patients and that treating these Enterovirus infections can lead to significant improvement and recovery.
Enteroviruses have been associated with ME since the 1930's. Names such as 'Epidemic Neuromyasthenia’, ‘Encephalitis’, ‘Akureyri Disease’, ‘atypical poliomyelitis’, 'Iceland disease', ‘poliomyelitis-like epidemic neuromyasthenia’ ‘Abortive Poliomyelitis’ were used to describe the illness prior to the term ‘Myalgic Encephalomyelitis’ being created by Dr. Melvin Ramsey in 1956. Enteroviruses were implicated in most epidemics from the 1930's to the present day.
His research paper provides some important insights - Chronic fatigue syndrome is associated with chronic enterovirus infection of the stomach.
Chia JK, Chia AY.
J Clin Pathol. 2008 Jan;61(1):43-8. Epub 2007 Sep 1. See diagram below:
Dr. John Chia presents his research findings up to the year 2011 to the National Institutes of Health (NIH) in the USA below:
Dr. Chia's work and findings are similar to those of John Richardson, a medical doctor who was based in Newcastle in England who treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.
The outbreak in Iceland was important, and provided some vital clues about the illness and the role of Enteroviruses.
"However,
children
in epidemic Neuromyasthenia areas
responded
to
poliomyelitis
vaccination
with
higher
antibody titres
than
in
other
areas
not
affected
by
the
poliomyelitis
epidemic,
as
if
these
children
had
already
been
exposed
to
an
agent
immunologically
similar
to
poliomyelitis
virus
(Sigurdsson,
Gudnad6ttir Petursson,
1958).
Thus,
the
agent
responsible
for
epidemic Neuromyasthenia would
appear
to
be
able
to
inhibit
the
pathological
effects
of
poliomyelitis
infection.
When
an
American
airman
was
affected
in
the
1955
epidemic
and
returned
home,
a
similar
secondary
epidemic
occurred
in
Pittsfield,
Massachusetts,
U.S.A.
(Hart,
1969:
Henderson
and
Shelokov,
1959)."
Many outbreaks of ME or epidemic Neuromyasthenia worldwide followed an outbreak of polio virus.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
Dr. Chia also presents his medical experiences in the videos below:
Dr. Kenny De Meirleir is medical doctor based in Belgium and in Nevada in the USA. He runs a well known medical clinic in Belgium and also works for the Whittemore Peterson Institute in Nevada in the USA. He has been treating ME patients and researching the illness since 1990. He has seen thousands of ME patients over the years. The medical and scientific findings of Dr. Kenny De Meirleir over 20 years support the role of infections and immune system abnormalities in ME . Lecture series by Dr. Kenny De Meirleir videos 1 - 20, created in 2012 and 2013. Specifically for medical doctors and hospital consultants.
Commentary & Discussion
Infections and immune system abnormalities in ME
Dr. Lucinda Bateman. Dr. Bateman is a highly respected and well experienced medical doctor who has been treating ME patients since the late 1990's. She is a medical graduate of the prestigious Johns Hopkins University in Maryland. Dr. Bateman runs an ME clinic in Utah in the USA which is visited by patients from many states throughout the USA. Her expertise in ME has been ackowledged by the US Government authorities and national patient organistions in the USA, who have asked her to serve on their committees and expert bodies.
Dr. Martin Lerner is a medical doctor with 40 years experience. Certified by the American Board of Internal Medicine and is an Infectious Disease Specialist. Residency, Internal Medicine, Harvard Medical Services. Boston City Hospital and Barnes Hospital, St. Louis, MO. Washington University School of Medicine, M.D. Two Years, National Institute of Allergy and Infectious Diseases, Epidemiology Unit.
Alumni Awardee, Washington University School of Medicine.
Three years research fellow in infectious diseases at the Thorndike Memorial Laboratory, Boston City Hospital and Harvard Medical School under the direction of *Dr. Maxwell Finland, (founder of subspecialty infectious diseases). Chief of the Division of Infectious Diseases and Professor of Internal Medicine at Wayne State University School of Medicine, 1963-1982. Established a clinical virology laboratory and trained 33 physicians in the subspecialty of infectious diseases, Wayne State University, 1963-1982.
IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA Daniel Peterson, M.D., Griffith University, Gold Coast, Australia, Owner, Sierra Internal Medicine, Incline Village, NV Sonya Marshall - Gradisnik, BSc (Hons), Ph.D. , Professor of Immunology, Director, National Centre for Neuroimmunology & Emerging Diseases, Griffith University, Australia Sharni Hardcastle, Ph.D., Research Assistant and Practical Demonstrator , Bond University, Gold Coast, Australia Nancy Klimas, M.D. Ph.D., Professor of Medicine and Director, NSU COM Institute for Neuro-Immune Medicine Director, Miami VAMC Gulf War Illness and ME Research Program Paula Waziry, Ph.D, Assistant Professor, Neuro Immune Medicine, COM, Nova Southeastern University, Miami, Fl Konstance Knox, Ph.D., Founder, CEO, Coppe Healthcare Solutions David Baewer, M.D. Ph.D, Medical Director, Coppe Healthcare Solutions Isabel Barao, Ph.D., Research Assistant Professor, University of Nevada, Reno, Simmaron Research Scientific Gunnar Gottschalk, B.S., Simmaron Research, Incline Village, NV Troy Querec, Ph.D., Associate Service Fellow, Centers for Disease Control and Prevention, Atlanta, GA Dennis Mangan, Ph.D., Chair, Trans-NIH ME Research Working Group, Office of Research on Women's Health, U.S. National Institutes of Health Mary Ann Fletcher, Ph.D., University of Miami Miller School of Medicine Professor of Medicine, Microbiology/Immunology and Psychology Elizabeth Unger, M.D. Ph.D., Chief, Chronic Viral Disease Branch, Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases. Centers for Disease Control and Prevention, Atlanta, GA
Dr. Sarah Myhill is a distinguished and highly regarded medical doctor and researcher based in Wales. She runs the famous Myhill Clinic there. Dr. Myhill has been treating ME patients and researching the illness since the mid 1990's. Her team's collaboration with Oxford University researchers into Mitochondria has been revolutionary and provided important new medical insights into Mitochondria and their role in illness and disease.
The following video lecture was presented by Dr. Sarah Myhill in 2014. Her areas of speciality are the mitochondria, oxidative stress, toxins, and the immune system, and the inter-relationship between them in ME patients. She provides a brilliant analysis of these areas and provides some useful diagnostics and treatments for patients.
Dr. Jose Montoya is a medical doctor and a Professor in Stanford University Medical School in the USA. He has been treating ME and researching the illness since 2000. His work concentrates on viral and pathogen infections and immune dysfunctions in ME .
Dr. Garth Nicolson is a professional scientific researcher based in Florida, USA. He has been researching pathogen infections and immune dysfunctions since the late 1980's. He runs the Institute for Molecular Medicine, and has carried out extensive research on hundreds of ME patients over the years. The scientific and medical findings of Dr. Garth Nicolson (USA) has consistently found that high percentages of ME patients have mycoplasma infections. A significant percentage also have co-infections including HHV6a and various bacteria infections. This correlates to illness severity. Dr. Nicolson also found evidence of immune dysfunctions. This ties into the work of other scientists and doctors who have consistently found viral, mycoplasma and other pathogen infections, along with immune dysfunction in ME patients.
Dr. Malcolm Hooper is a British Pharmacist and emeritus professor of medicinal chemistry at the University of Sunderland in Britain. He has researched and published many papers on ME and Gulf War illness. He is Chief Scientific Adviser to the British Gulf War Veterans Association. He is the medical advisor for The Grace Charity for ME in Britain.
Video Lectures by Dr. Malcom Hooper. Videos 1 - 10
Dr. Ritchie Shoemaker is a medical doctor based in Maryland, USA. He is one of the top experts on mycotoxins in the world. He has been treating ME patients since the late 1990's, and he believes that myctoxins are a major factor in some ME subgroups and in other illnesses. Mycotoxins are accepted by the CDC and NIH in the USA as being hazardous to health. Lecture below on the effects of chronic myoctoxins and mold exposure on the immune system, endocrine system and nervous system.
Dr. Paul Cheney, Dr. De Meirleir and Dr. Peterson (mentioned above) are now using tests for mycotoxins as part of their diagnostics protocol for ME .
Dr. Andrew Campbell is a medical doctor who has seen ME patients since the late 1990's. He believes that myctoxins are a major factor in some ME subgroups and in other illnesses. Mycotoxins are accepted by the CDC and NIH in the USA as being hazardous to health. Lecture below on the effects of chronic myoctoxins and mold exposure on the immune system, endocrine system and nervous system.
Dr. Paul Cheney, Dr. De Meirleir and Dr. Peterson (mentioned above) are now using tests for mycotoxins as part of their diagnostics protocol for ME .
7. Research Findings
Summary of Research Findings The scientific research, much of it catalogued above and in the Scientific Evidence Section, shows that ME is Multi-Factor illness, a chronic disabling physical illness, which involves multiple biological dysfunctions and abnormalities.
According to gene studies and other biological studies, there are at least 5 subgroups in ME . Many patients also have co-existing illnesses. We are dealing with a high level of biological complexity here. The research strongly suggests the illness involves the following
Primary biological dysfunction and abnormality
(1) ATP, Mitochondria & Krebs cycle dysfunctions, including destruction of Mitochondria
The research and clinical work of Dr. Sarah Myhill, Dr. Behan and Dr. Paul Cheney and other doctors and researchers have consistently found this biological abnormality. Deficient ATP produced and deficient recycling of ATP. A rapid shift to anerobic metabolism, build up of lactic acid, purines, muscle pains etc. during and after exercise, and post-exercise malaise commonly found in ME patients. Oxidative & Nitrosative stress damage to inner & outer membranes of mitochondria, cristae, proteins, and DNA of mitochondria. Krebs cycle blocks. Redox failure. Ion channel interruption & dysfunctions affecting Ca. Mg. and K levels. Deficient Electron Transport Chain. Impaired ATP production and Oxidative Phosphorylation. Impaired Translocator protein activity. Acceleration of AMP & glycolysis. This may be due to chronic infections, a chronically activated inflammatory immune system, hypoxia or lack of oxygen in cells, toxins and the high levels of oxidative and nitrosative stress in the illness. It is known by scientists that some viruses such as EBV, other herpes viruses and retroviruses and bacteria such as mycoplasma and Borrelia (Lyme disease) can interfere with, disrupt and destroy the mitochondria. These infections are regularly found in ME and CFS patients.
Mitochondria dysfunction and destruction is the most important factor as the mitochondria and krebs cycle produces ATP, which is fuel or energy for the immune system, the nervous system, the brain, the muscles, the heart, the glands, and all the organs. Any significant deficiency in ATP will cause a slow down in the activity of these organs and the body, and more serious deficiencies can cause extreme tiredness and fatigue most or all of the time. This mitochondria damage over time may also explain Cardiac dysfunctions in ME.
(2) Immune system dysfunctions and deficiencies caused by or accompanied by viral / mycoplasma / pathogen infection (active and latent) and/or toxins. Overactive 2'-5' oligosynthetase pathway, defects in the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway with effects on immune system function and important ion channels. In the case of the 2-5a synthetase / RnaseL anti-viral pathway, it is believed that human leukocyte elastase and/or calpain cleaves the 80 kDa form of RnaseL into 37 kDa RnaseL, cleaves STAT1-alpha protein and p53 protein and Actin, bringing about deficiencies in these proteins. These proteins are essential for normal immune system function, and their depletion and abscence leads to serious and continuing immune system dysfunction. These abnormalities strongly indicate an immune system which is being activated by chronic viral infection, and the immune system is becoming depleted or defective over time.
There is an accompanying increase in NF-Kb levels and activity which is pro-inflammatory. Low numbers of NK cells and reduced NK cell function and cytotoxicity. The Rituximab studies show that B cell abnormalities, including excessive levels of defective B cells are a major factor and may perpetuate the illness. Scientists such as Pender and others believe that chronic EBV infection of B cells plays a role in ME, CFS and other autoimmune illnesses. Chronic immune system activation with dominance of pro-inflammatory cytokines. T cell abnormalities, including depleted Suppressor cells, CD8 and T reg cell abnormalities and an abnormal CD4/CD8 ratio. Retrovirus infections have been found in ME patients, and these infections can deplete T cell suppressor cells and other T cell subsets. Interferon poisoning in some subgroups of patients, and this is is also linked to viral infections. The overactive immune system is progressing to autoimmunity in some cases, there are HLA abnormalities and other evidence of autoimmunity in many patients. VDR abnormalities which weaken immunity, and increase susceptibility to chronic infection and autoimmune risk (Dr. Marshall, Marshall Protocol). Gastrointestinal abnormalities which contribute to immune system dysfunctions.
The immune system has a high demand for ATP in this illness, while ATP is being depleted through mitochondria destruction or degradation.
(3) the evidence from prior ME epidemics show that infections play a role in most ME patients. Top ME doctors A. Gilliam, Melvin Ramsay, Elizabeth Dowsett, John Richardson of Newcastle-upon-Tyne, W.H. Lyle, Elizabeth Bell, James Mowbray of St Mary’s, Peter Behan and Byron Hyde all believed that the majority of primary M.E. patients fell ill following exposure to an Enterovirus. Dr. John Richardson, a medical doctor based in Newcastle in England treated ME patients from many parts of Britain for over 40 years. He developed an expertise in diagnosing the illness, and became one of the world's foremost experts in ME. He even used autopsy results from dead patients to investigate the illness. He found that Enteroviruses and toxins played a major role in ME, and that this led to immune dysfunction, neurological abnormalities, endocrine dysfunction, and over time to increased risk of cardiac failure, cancers, carcinomas, and other organ failure. He wrote a book about his medical experiences called Enteroviral and Toxin Mediated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. This book is a classic medical book on the illness, and provides an excellent introduction to ME. Historically, Enterovirus infections mainly target the nervous system, brain, muscles and intestines, all of which abnormal in ME patients.
In subgroups, there is evidence of Retrovirus infection and Herpes infections and changes to cell structures and to T cell subsets. There is evidence for continuing viral, mycoplasma, bacteria and other pathogen infections (both active and latent, including partially latent) of the nervous system, nerve junctions, brain, immune system cells, intestines, joints, muscles, and other body organs. These infections may be causative, opportunistic or a co-factor in the illness. There are high levels of oxidative and nitrosative stress and inflammation, and cellular destruction, arising from chronic immune system activation, infections, immune system and cellular dysfunctions, and toxins.
Secondary
biological dysfunctions and abnormalities (1) dysfunctions of the central nervous system, the brain and the autonomic nervous system, and involves significant chronic inflammation, lesions, reductions in grey and white matter, brain hypoperfusion, increased ventricular lactate, spinal fluid abnormalities, autonomic dysfunctions and other abnormalities. This adversely affects many other body functions.
(2) Dr. Paul Cheney has found toxic build up in the body in many patients. Flow reversal in the liver and the brain. Chronic Cerbral Spinal Venous Insufficiency (CCSVI). Chronic He patic Venous Insufficiency (CHVI). Cardiac Dysfunction. This reversal leads to auto-intoxication and a build up of toxins and toxin related damage to cells, tissues, organs, glands, etc.. (Dr. Paul Cheney) (3) methylation cycle blocks and glutathione deficiency. The methylation cycle is important and produces many substrates and co-factors for other body organs and processes, including the mitochondria. Deficient glutathione increases oxidative and nitrosative stress and this contributes to mitochondria abnormalities and dysfunctions. (4) HPA axis dysfunctions, in particular hypothalmus gland, adrenal gland and thyroid gland dysfunctions and abnormal hormone output, which adversely affects hormones, sleep and immune function.
All of these 7 factors are the core of the illness, the perpetuating factors over time. Subgroups will contain most of the 7 factors mentioned above. There are slight differences between patient groups which are due to subgroups, genetic differences, different environment exposures and toxins, different infectious agents, different microbiome and metagenome status, and different diet and lifestyles. These abnormalities and dysfunctions have a domino effect on other cellular functions and body functions leading on to several other dysfunctions, and to severe illness.
The immune system dysfunctions and abnormalities in ME patients makes them more susceptible to various infections. The acquired infection(s) will depend on one's geographical location and exposures, and one's genetic status and immune system status. Some of the following pathogens have been consistently found in ME patients:
Viruses include: Reactivated (latent) EBV virus, particularly in B cells, nervous system, glands and organs, HHV6a virus, Herpes family viruses 1-8, Parvovirus B-19, CMV, Coxsackie viruses, Enteroviruses, Ross river virus, Q fever virus, Stealth virus, JHK virus, Parainfluenza Virus-5 (PIV-5), Paramyxovirus and measles viruses of the Paramyxoviridae family, Cryptovirus, Borna virus, HTLV family viruses, HGRV virus in spinal fluids, nerve tissues, blood, brain, intestines, and muscles. Retroviruses are important, as Retrovirus sequences were found in 85% of ME cases, and Anellovirus found in 75% of ME cases in research conducted by Dr. Hornig and Dr. Lipkin in Columbia University in September 2013. Most of these viruses listed here would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Reactivated latent viruses include EBV, HERV-K18, Varicella-Zoster virus, Herpes family viruses 1-8, measles viruses of the Paramyxoviridae family. Some viral infections can reactivate latent viruses and undermine immune system functions. Mycoplasma: M. fermentans, M. penumoniae, M. hominis, M. penetrans, M. pirum, M. incognito. in intestines, spinal fluids, blood, brain, nerve tissues, muscles. These mycoplasmas would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Bacteria: Chronic Lyme disease, Ehrlichia, Bartonella, Brucella, Rickettsia, Chlamydia pneumonia, Staphylococcus spp. (live blood analysis), and Bacteria, including Microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms in spinal fluids, intestines, blood, brain, nerve tissues, muscles. Intestinal overgrowth of Gram positive D/L lactate-producing bacteria which are known to produce H2S (hydrogen sulfide) in the presence of certain heavy metals as a survival defense mechanism (Dr. Kenny De Meirleir). These bacteria would include chronic, low level, sub-acute infections which inflict damage and immune activation, but which may not show up in standard or outdated tests. Parasite: Cryptostrongylus pulmoni (rare cases), Babesia, Candida, Giardia lamblia, Aspergillus Niger Molds, Bacteria and Mycotoxins in water damaged buildings: Stachybotrys family of molds, Cladosporium, Penicillium, Alternaria, Aspergillus, mycobacteria, Actinomycetes, Lipopolysaccharides (LPS), Microbial Volatile Organic Compounds (VOCs), Hemolysins.
These can cause chronic inflammatory immune response and immune dysfunction over time.
These infections may be causative, opportunistic or a co-factor in the illness.
Most patients are infected with EBV and suffered mononucleosis at some stage in their life. Over 90% of adults carry one or more herpes viruses for life. Latent infections can last a human lifetime (80 -100 years). EBV goes into a latent stage after active infection, and tends to live inside B cells. It can also live in other body organs. EBV uses the machinery of the B cells to replicate itself and to migrate to other body parts. The infected and abnormal B cells is a key factor in this illness. These deep infections of immune cells and body organs along with molecular mimicry can create conditons of autoimmunity which are directly related to the site of EBV infection. Chronic EBV infection and other Herpes infection or latent incubation in the liver, the spleen, the thyroid gland, the joints, adrenal glands and the nervous system can lead to variety of autoimmune conditions, which can confuse doctors.
EBV (and other Herpes viruses) may be able to undermine the effectiveness of CD8 T cells and NK cells and the TH1 cytokine system, which are the body's main defence against viruses and bacteria. These immune deficiencies are regularly found in ME and CFS and other autoimmune illnesses.
Rituximab, B-cell abnormalities & Viral induced Autoimmunity & Cancers
The scientific findings show that B-cell abnormalities play a significant role in autoimmunity in ME, and the success of the drug Rituximab confirms these findings. The scientific research of Fluge and Mella in Norway show that depleting B-cells through Rituximab brings about recoveries in two thirds of patients. Yet this takes several months to achieve. Once Rituximab is withdrawn, the patients become ill again after a few months, as B-cell numbers increase. Viruses / mycoplasmas may be hiding in B-cells so as to infect patients and/or increasing B-cell production for infection purposes, indirectly causing both an autoimmune response and an ongoing infection. Dr. Martin Lerner (Michigan, USA) believes that anti-virals kill the viruses, but do not hit the B-cells which incubate the virus(es) and that Rituximab hits the B-cells, but has little effect on the viruses. This would explain why Rituximab improves ME patients after a few months, but when Rituximab is stopped, the patients deteriorate, as (infected) B cell populations increase again. Dr. Michael Pender in his paper CD8+ T-Cell Deficiency, Epstein-Barr Virus Infection, Vitamin D Deficiency, and Steps to Autoimmunity: A Unifying Hypothesis. Pender MP. Autoimmune Dis. 2012;2012:189096. postulates that EBV virus is capable of living inside B cells and using the machinery of these cells to replicate itself, and cause continuing infection, autoimmunity and immune dysfunction which could last for years and decades. He also states that reduced cytotoxic T cell function plays a key role in this, allowing EBV infection of B cells and other cells to continue. This is explored further in the following papers Could the Epstein-Barr Virus – Autoimmunity Hypothesis Help Explain Chronic Fatigue Syndrome ? and EBV I: A Deficient Immune Response, Increased Levels of Epstein-Barr Virus Opens Up EBV Question in Chronic Fatigue Syndrome Again. An excellent scientific paper produced by scientific researchers in Germany in 2014 shows the importance of chronic EBV infection, including persistent reactivation of latent EBV combined with a defective immune system. This plays a major role in ME (Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome.
Loebel M, Strohschein K, Giannini C, Koelsch U, Bauer S, Doebis C, Thomas S, Unterwalder N, von Baehr V, Reinke P, Knops M, Hanitsch LG, Meisel C, Volk HD, Scheibenbogen. Scientific analysis and discussion on http://simmaronresearch.com/2014/03/1591/ )
Listing of Research findings and papers worldwideand categorisation of biological abnormalities and dysfunctions and infections found in ME
The following paper by the organisation Paradigm Change details many of the biological abnormalities, dysfunctions and infections found in ME and CFS patients and research papers to support this. ME and Medical Abnormalities - Medical Research paper.
The Dubbo Studies which were published in leading medical journals verify much of the above, and point to genetic factors, environmental factors and a post-infectious dysfunctional immune system as being the key factors in ME .
(ii) Phases or Stages of the Illness The phase of the illness will affect biomarkers and the immune system subsets. These can change over time. Tests on 285 ME patients and 200 controls in 2013 by Hornig et al. in New York show that there are significant differences in biomarkers between patients who have the illness for 3 years or less, and those who have it for more than 3 years. This explains the slight differences between patient groups which consistently appear in scientific studies. (Preliminary findings of Hornig et al., September 2013). This ties in to the findings of Dr. Paul Cheney who has stated there are 3 phases of the illness - phase 1, 2, 3. This is important as ME progresses over time, and the patient usually develops multiple biological dysfunctions and abnormalities and can become very disabled.
Dr. Paul Cheney has successfully treated hundreds of ME patients in the USA since the early 1990's has identified 3 phases of the illness in the following lectures Lecture by Dr. Paul Cheney who has successfully treated hundreds of ME patients in the USA Summary of the above lecture by Dr. Paul Cheney
What phase is the patient in, how long does he/she have the illness ? is the patient in remission or having a relapse ? is the patient severely ill, moderately ill or mildly ill. These will affect immune system subsets and other biological markers.
Overview of Immune System markers and associated Genetic markers in ME The following video of a lecture by Dr. Gordon Broderick, University of Alberta presents the immune system findings and underlying genes involved in this illness
There have been well documented ME epidemics and outbreaks throughout history. These include the following:
1917 Van Economo reports an illness involving brain and neurological inflammation and great fatigue and some deaths. See paper 'New Clinical Entity' published in the Lancet in 1956.
1918 - 1924, several outbreaks of an illness involving brain and neurological inflammation and fatigue reported throughout Europe. See paper 'New Clinical Entity' published in the Lancet in 1956.
1924 England and Wales 5,039 cases of encephalitis lethargica. See paper 'New Clinical Entity' published in the Lancet in 1956.
1934
Los Angeles County Hospital. Called 'Atypical Poliomyelitis'
1936
Fond Du Lac, Wisconsin - St. Agnes Convent - Encephalitis
1937
Erstfeld, Switzerland -
Abortive Poliomyelitis
1937
St. Gallen, Switzerland
- Frohburg Hospital – Abortive Poliomyelitis
1939
Middlesex, England - Harefield Sanatorium
1939
Degersheim, Switzerland - Abortive Poliomyelitis
1945
Pennsylvania. Hospital of the University of Pennsylvania - epidemic Pleurodynia
1946
Iceland
disease resembling Poliomyelitis with the character of Akureyri disease
1948
Iceland, North Coast towns - epidemic simulating Poliomyelitis
The outbreak in Iceland was important, and provided some vital clues about the illness.
"However,
children
in epidemic Neuromyasthenia areas
responded
to
poliomyelitis
vaccination
with
higher
antibody titres
than
in
other
areas
not
affected
by
the
poliomyelitis
epidemic,
as
if
these
children
had
already
been
exposed
to
an
agent
immunologically
similar
to
poliomyelitis
virus
(Sigurdsson,
Gudnad6ttir Petursson,
1958).
Thus,
the
agent
responsible
for
epidemic Neuromyasthenia would
appear
to
be
able
to
inhibit
the
pathological
effects
of
poliomyelitis
infection.
When
an
American
airman
was
affected
in
the
1955
epidemic
and
returned
home,
a
similar
secondary
epidemic
occurred
in
Pittsfield,
Massachusetts,
U.S.A.
(Hart,
1969:
Henderson
and
Shelokov,
1959)."
Many outbreaks of ME or epidemic Neuromyasthenia worldwide followed an outbreak of polio virus.
Parish JG (1978), Early outbreaks of 'epidemic neuromyasthenia', Postgraduate Medical Journal, Nov;54(637):711-7, PMID: 370810.
1948 300
sporadic
cases
of
epidemic Neuromyasthenia
seen
in
South
California
between
1948
and
1965.
1949
Adelaide, South Australia - a disease resembling Poliomyelitis
1949 Cambridgeshire, England -
aberrant poliomyelitis. Involvement of other Enteroviruses suspected.
1950
Louisville, Kentucky -- St. Joseph
's Infirmary - epidemic Neuromyasthenia
1950
Upper State New York -- outbreak resembling the
Iceland disease, simulating
"
acute Anterior Poliomyelitis
1952
London, England - Middlesex Hospital Nurses
'
Home - Encephalomyelitis
associated with Poliomyelitis virus
1952
Copenhagen, Denmark - epidemic Myositis
1952
Lakeland, Florida - epidemic Neuromyasthenia
1953
Coventry and District, England - an illness resembling Poliomyelitis observed in
nurses
1953
Rockville, Maryland - Chestnut Lodge Hospital - Poliomyelitis-like epidemic
Neuromyasthenia
1953
Jutland, Denmark - epidemic Encephalitis with vertigo
1954 Tallahassee, Florida - epidemic Neuromyasthenia
1954 Seward, Alaska - benign Myalgic Encephalomyelitis (Iceland Disease)
1954
Berlin, Germany - British army - further outbreak of a disease resembling
Poliomyelitis
1954
Liverpool, England - outbreak among medical and nursing staff in a local
hospital
1954 Johannesburg,
South
Africa - epidemic Neuromyasthenia
1955
Dalston, Cumbria, England – epidemic and sporadic outbreak of an unusual
disease
1955
London, England - Royal Free Hospital - outbreak in staff and patients of Benign
Myalgic Encephalomyelitis
1955 Hampstead, London
1955
Perth, Australia - virus epidemic in waves
1955
Gilfac Goch, Wales - outbreak of benign Myalgic Encephalomyelitis
1955
Durban City, South Africa - Addington Hospital. Outbreak among nurses called 'Durban Mystery Disease' also called 'epidemic Neuromyasthenia'
1955
Segbwema, Sierra Leone - outbreak of Encephalomyelitis
1955
Patreksfjorour and Porshofn, Iceland - unusual response to polio vaccine
1955
Northwest London, England - nurses
'
residential home - acute Infective
Encephalomyelitis simulating poliomyelitis
1956
Ridgefield, Connecticut - epidemic Neuromyasthenia
1956
Punta Gorda Florida - outbreak of epidemic Neuromyasthenia
1956
Newton-le-Willows, Lancashire, England - Lymphocytic Meningoencephalitis with
myalgia and rash
1956
Pittsfield and Williamstown, Massachusetts - benign Myalgic Encephalomyelitis
1956
Coventry, England - epidemic malaise, benign Myalgic Encephalomyelitis
1957
Brighton, South Australia - Cocksakie Echo virus Meningitis, epidemic Myalgic
Encephalomyelitis
1958
Athens, Greece - nurses
'
school - outbreak of benign Myalgic Encephalomyelitis
with periostitis and arthopathy noted.
1958
Southwest London, England - reports of sporadic cases of Myalgic
Encephalomyelitis
1959
Newcastle Upon Tyne, England - outbreak of benign Myalgic Encephalomyelitis
1961
Basel, Switzerland - sporadic cases of benign Myalgic Encephalomyelitis
1961
New York State - outbreak of epidemic Neuromyasthenia in a convent
1964
Northwest London, England - epidemic malaise, epidemic Neuromyasthenia
1964
Franklin, Kentucky - outbreak of Neuromyasthenia in a factory
1965 Lamarque,
Texas,
U.S.A.
- epidemic Neuromyasthenia. Investigated by Leon-Sotomayor
(1969).
1967
Edinburgh, Scotland - sporadic cases resembling benign Myalgic
Encephalomyelitis
1968
"
Fraidek, Lebanon - benign Myalgic Encephalomyelitis
1969
Brooklyn, New York - State University of New York Downstate Medical Center -
epidemic Neuromyasthenia, unidentified symptom complex
1970
Lackland Air Force Base, Texas - epidemic Neuromyasthenia
1970
London, England - Great Ormond Street Hospital for Children - outbreak of
Neuromyasthenia among nurses
1975
Sacramento, California - Mercy San Juan Hospital - Infectious Venulitis, epidemic
"
Phelobodynia
1976
Southwest Ireland - epidemic Neuromyasthenia, benign Myalgic
Encephalomyelitis
1977
Dallas – Fort Worth, Texas - epidemic Neuromyasthenia
1979
Southampton, England - Myalgic Encephalomyelitis
1980
West Kilbridge, Ayrshire, Scotland - epidemic Myalgic Encephalomyelitis
1980
San Francisco, California – epidemic persistent flu-like illness
1981
Stirlingshire, Scotland
- sporadic Myalgic Encephalomyelitis
1982
West Otago, Dunedin and Hamilton, New Zealand - Myalgic Encephalomyelitis
1983
Los Angeles, California - initial cases of an unknown, chronic symptom complex
involving profound "fatigue"
1984
Lake Tahoe Area of California/Nevada - start of a yearlong epidemic involving
"
over 160 cases of chronic illness eventually characterized as Chronic Fatigue
Syndrome Source: Paradigm Change web site
ME has several subgroups, and each subgroup contains some of the above biological abnormalities, dysfunctions and infections mentioned above.
The Dubbo Studies which were published in leading medical journals point to genetic factors, environmental factors and a post-infectious dysfunctional immune system as being the key factors in ME .
Overview of Immune System markers and associated Genetic markers in ME The following video of a lecture by Dr. Gordon Broderick, University of Alberta presents the immune system findings and underlying genes involved in this illness
Phases or Stages of the Illness The phase of the illness will affect biomarkers and the immune system subsets. These can change over time. Tests on 285 ME patients and 200 controls in 2013 by Hornig et al. in New York show that there are significant differences in biomarkers between patients who have the illness for 3 years or less, and those who have it for more than 3 years. This explains the slight differences between patient groups which consistently appear in scientific studies. (Preliminary findings of Hornig et al., September 2013). This ties in to the findings of Dr. Paul Cheney who has stated there are 3 phases of the illness - phase 1, 2, 3. This is important as ME progresses over time, and the patient usually develops multiple biological dysfunctions and abnormalities and can become very disabled.
Dr. Paul Cheney has treated thousands of ME patients in the USA since the early 1990's has identified 3 phases of the illness in the following lectures Lecture by Dr. Paul Cheney who has successfully treated hundreds of ME patients in the USA Summary of the above lecture by Dr. Paul Cheney
Further corroborating scientific evidence of viral infections and bacteria infections in ME is provided by Harvard Medical School Professor Anthony Komaroff and Neurologist Tracey Cho in their paper ' Role of Infection and Neurologic Dysfunction in Chronic Fatigue Syndrome.' Anthony L. Komaroff, Tracey A. Cho. Semin Neurol 2011; 31(3): 325-337.
IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA Daniel Peterson, M.D., Griffith University, Gold Coast, Australia, Owner, Sierra Internal Medicine, Incline Village, NV Sonya Marshall - Gradisnik, BSc (Hons), Ph.D. , Professor of Immunology, Director, National Centre for Neuroimmunology & Emerging Diseases, Griffith University, Australia Sharni Hardcastle, Ph.D., Research Assistant and Practical Demonstrator , Bond University, Gold Coast, Australia Nancy Klimas, M.D. Ph.D., Professor of Medicine and Director, NSU COM Institute for Neuro-Immune Medicine Director, Miami VAMC Gulf War Illness and ME Research Program Paula Waziry, Ph.D, Assistant Professor, Neuro Immune Medicine, COM, Nova Southeastern University, Miami, Fl Konstance Knox, Ph.D., Founder, CEO, Coppe Healthcare Solutions David Baewer, M.D. Ph.D, Medical Director, Coppe Healthcare Solutions Isabel Barao, Ph.D., Research Assistant Professor, University of Nevada, Reno, Simmaron Research Scientific Gunnar Gottschalk, B.S., Simmaron Research, Incline Village, NV Troy Querec, Ph.D., Associate Service Fellow, Centers for Disease Control and Prevention, Atlanta, GA Dennis Mangan, Ph.D., Chair, Trans-NIH ME Research Working Group, Office of Research on Women's Health, U.S. National Institutes of Health Mary Ann Fletcher, Ph.D., University of Miami Miller School of Medicine Professor of Medicine, Microbiology/Immunology and Psychology Elizabeth Unger, M.D. Ph.D., Chief, Chronic Viral Disease Branch, Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases. Centers for Disease Control and Prevention, Atlanta, GA
Morris et al. Model of ME
Activated immune pathways and inflammatory cytokines and inflammatory markers, and neuroinflammation, and high oxidative and nitrosative stress levels and damage, and mitochondria damage, damage to the nervous system, with or without infection(s) has been found in neurodegenerative diseases such as Parkinsons, Alzheimers, MS and many others. This causes extreme fatigue and tiredness. This is also found in autoimmune diseases. And they are also found in ME, a neurological illness according to WHO, with immune system dysfunctions.
Morris G, Maes M. Oxidative and nitrosative stress and immune-inflammatory pathways in patients with Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Curr Neuropharmacol. 2014;12:168–85.
Morris G, Anderson G, Galecki P, Berk M, Maes M. A narrative review on the similarities and dissimilarities between myalgic encephalomyelitis/chronic fatigue syndrome (ME) and sickness behavior. BMC Med. 2013;11:64.
Morris G, Maes M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab Brain Dis 2014;29(1):19–36
There have been many research findings and clinical findings which show the harmful effects of CBT and GET and exertion in ME patients. In addition to this, the inefficacy of CBT and GET in terms of lack of full recovery, lack of return to normal function, lack of normal health (prior to illness), lack of return to sporting and other social activities, lack of return to full time employment or full time education or training has also been shown. This research is listed in the links below