Immune System Dysfunctions and Abnormalities, including Deficient Immune Response to Infections
- Tests mentioned by International Consensus criteria 2011 and Canadian criteria 2003
-
Test for abnormalities in the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway
- Immune system related Genes
- Test for chronic inflammatory immune response to molds, mycobacteria and mycotoxins
- Immune system subsets
- NK cells, T cells, Cytokines, B cells
-
Vaccines - test for Adverse Immune System reactions to vaccines
- Tests for Autoimmune Disorders including autoimmune marker mimcry by viruses
- Test for Protein M
- Test for Methylation Blockage
- Test for Toxin damage to the Immune system
- Test for Vitamin D deficiency and B-12 Deficiency
- Test for Intestinal bacteria associated with normal Immune system functions
- Lymphatic Drainage Tests
- Other Immune Dysfunction tests
The research and evidence cited above points convincingly to a number of immune dysfunctions and autoimmune disorders in addition to infection by viruses, bacteria and pathogens in subgroups of ME patients. It is important to diagnose the immune dysfunctions and infections present in ME patients, subgroup the patients, and administer appropriate medical treatments to the subgroups.
Phases or Stages of the Illness The phase of the illness will affect biomarkers and the immune system subsets. These can change over time. Tests on 285 ME patients and 200 controls in 2013 by Hornig et al. in New York show that there are significant differences in biomarkers between patients who have the illness for 3 years or less, and those who have it for more than 3 years. This explains the slight differences between patient groups which consistently appear in scientific studies. (Findings of Hornig et al., September 2013).
There are significant cytokine differences between patients who have the illness for 3 years or less and those who have it for 3 years or more. The p values in this research are less than 0.05 in many cases, with several less than 0.01, proving that several cytokines are playing an important role in the illness. This is one of the most important findings in recent years. Pro-inflammatory cytokines are increased in the plasma in early phase ME/CFS. Plasma TH2/counter-regulatory cytokines are also increased in early phase ME/CFS. IFNy and IL12p40 are markedly upregulated in early phase ME/CFS. Interferon gamma is quite significant with a p value of .001. Hornig et al.. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. 27 February 2015, Sci. Adv. 1, e1400121 (2015) DOI: 10.1126/sciadv.1400121
The Chronic Fatigue Initiative (CFI)- Findings from the CFI Cohort Study and Pathogen Discovery & Pathogenesis Project IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
This ties in to the findings of Dr. Paul Cheney who has stated there are 3 phases of the illness - phase 1, 2, 3. This is important as ME progresses over time, and the patient usually develops multiple biological dysfunctions and abnormalities and can become very disabled.
Dr. Paul Cheney has treated thousands of ME patients in the USA since the early 1990's has identified 3 phases of the illness in the following lectures Lecture by Dr. Paul Cheney who has successfully treated hundreds of ME patients in the USA Summary of the above lecture by Dr. Paul Cheney
The following factors will affect immune system subsets and other biological markers - does the person have ME or some other similar illness ? what phase is the patient in, how long does he/she have the illness ? is the patient in remission or having a relapse ? does the patient have a co-morbid or co-existing illness with ME ? what infections does the patient have and where are they located ? the patient's genetic weaknesses ? is the patient severely ill, moderately ill or mildly ill. Was it gradual onset ME or rapid onset ?
The RnaseL abnormality and
STAT1-alpha and p53 deficiencies and PKR abnormality are consistently found in most
CFS patients, typically 60% or more of CFS patients. The
scientific
research findings carried by Suhadolnik, Dr. Kenny De
Meirleir, Patrick Englebienne and De Becker all suggest that this
is the main factor in ME . Our Scientific
Research section and Kenny De Meirleir's book Chronic Fatigue Syndrome: A Biological Approach has numerous references to this. These
abnormalities may be the result of the immune system's response to
a past or continuing viral or mycoplasma infection or to toxins. In other
words, the immune system is stuck in a self-destructive phase as a
result of trying to destroy a viral or mycoplasma infection in the
past (or present).
Ampligen is one of three medical drugs (the others being Rituximab and Valganciclovir) which has
successfully treated CFS patients in scientific trials, and Ampligen targets this RnaseL
abnormality. Ampligen is available on prescription in Canada and
Mexico and is awaiting approval by the FDA in the USA. It is vitally important for all ME patients to carry
out the following tests. Tests for the 2-5a synthetase / RnaseL anti-viral pathway & PKR pathway
(i) Ratio of 37 kDa RnaseL to 80 kDa form of RnaseL. This measures the cleavage of the 80 kDa form of RnaseL
into 37 kDa RnaseL. An important diagnostic bio-marker. The ratio of the 37 kDa to
80 kDa RNase-L is reported to correspond
to a patient’s clinical status. The ratio of 37 kDa to the
normal 80 kDa form of RNase-L is high in
CFS patients. (1)
(ii) Upregulation of RNase L
enzyme activity. This can be 1,500 times
above normal levels in seriously ill CFS
patients.
(iii) the levels of
STAT1-alpha protein. Deviation from normal levels. Another important bio-marker. (1) (iv)low levels of
p53 protein. Deviation from normal levels. Another important bio-marker. (1) (v) Increased NF-Kb levels and activity. Another important bio-marker. (1) (vi) CD19 B-cell counts (vii) Elevated levels or over-active human luekocyte elastase - research findings suggest that elastase plays a key role
in the cleavage of RnaseL,
STAT1-alpha and p53 proteins and Actin and in arterial stiffness, and blood circulation problems. Tests carried out by Dr.
Kenny De Meirleir seem to confirm that elastase is the main
culprit in CFS (1) (viii) the cleavage of RnaseL
leads to the presence of RnaseL fragments. 3 RnaseL fragments have been found to be
significant: (1) Fragment 1, an ankyrin binding repeat domain which is known to
interact with various transport proteins. It is is capable of NF-kappaB mimicry. This may be interrupting the ion channels in the body.
"these results show that upon pathological cleavage of RNase L, fragments containing the ankyrin domain are released, which could be capable of interacting with selected members of the human ABC superfamily, preventing their interaction with the normal cognate ankyrin protein and hence impairing their proper cellular function. This interaction constitutes a common physiological mechanism explaining numerous and currently unexplained symptoms experienced by patients with CFIDS, which are otherwise totally unrelated."
Source: Interactions Between Rnase L Ankyrin-Like Domain and ABC Transporters as a Possible Origin for Pain, Ion Transport, CNS and Immune Disorders of Chronic Fatigue Immune Dysfunction Syndrome. Englebienne et al. 2001. Fragment 2, the 2-5A binding fragment that has catalytic
activity and thus is able to degrade RNA ; Fragment 3, shares homology with chain A of Cdk6 (Cyclin dependent
kinase). It of Cdk6 chain A mimicry ;
(ix) Cell Apoptosis (cell death) increases initially
in CFS and then is inhibited when the levels of Rnase L related
fragments reach a certain point ;(1) (x) Elevated levels or over-active protease levels. Elevated levels or over-active other proteolytic enzyme levels (1) (xi) abnormal cleavage of Actin (1) (xii) Elevated levels or over-active calpain levels; (1) (xiii) abnormal caspase activity and disrupted cell
apoptic process(1) (xiv) PKR activity and levels. Deviation from normal levels (1) (xv) Ion channel interruption and dysfunction affecting many other body parts. (xvi) Elastase, cathepsin-G and m-calpain are responsible for fragmenting RnaseL. Test for high concentrations and activity levels of these.
Channelopathy tests
Test for Channelopathy & Disturbance in the way certain ions (mainly sodium and potassium
salts) are transported in and out of cells across the cell membranes.
Serpin
Upregulation of Serpin in ME patients. This is important in the context of viral infection, immune dysfunction, RnaseL abnormality and elastase activity (Findings of Hornig et al., September 2013).
The following labs carry out these special tests:
Redlabs in Belgium is the leading laboratory in the world for these tests - http://www.redlabs.be
3. Marshall Protocol tests
Test for VDR blockage. This has multiple effects on the immune system leaving it more vulnerable to viral, bacteria and other pathogen infections, including microbiota of bacteria which include L-form, biofilm, and intracellular bacterial forms. See http://mpkb.org/home/mp
4. Test for chronic inflammatory immune response to molds, mycobacteria and mycotoxins
Myoctoxins have been found in high percentages of ME patients. One study found that 93% of ME patients had mycotoxin exposure, with many having multiple mycotoxin exposures, while none of the healthy controls had evidence of mycotoxin exposure. Mycotoxin exposure has been proven to lead to immune activation, in particular a chronic inflammatory state, and to endocrine system and nervous system abnormalities all which are consistently found in ME patients. Dr. Paul Cheney, Dr. De Meirleir and Dr. Peterson are now using tests for mycotoxins as part of their diagnostics protocol for ME / CFS. See Section - Tests for chronic inflammatory immune response to molds and mycotoxins
Dr. Mady Hornig and her research team at Columbia University, New York has found that there are significant cytokine differences between patients who have the illness for 3 years or less and those who have it for 3 years or more. The p values in this research are less than 0.05 in many cases, with several less than 0.01, proving that several cytokines are playing an important role in the illness. This is one of the most important findings in recent years. Pro-inflammatory cytokines are increased in the plasma in early phase ME/CFS. Plasma TH2/counter-regulatory cytokines are also increased in early phase ME/CFS. IFNy and IL12p40 are markedly upregulated in early phase ME/CFS. Interferon gamma is quite significant with a p value of .001.
Hornig et al.. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. 27 February 2015, Sci. Adv. 1, e1400121 (2015) DOI: 10.1126/sciadv.1400121
6.B-cells, Autoimmunity & Rituximab studies - abnormalities and possible infection of B cells
ME/CFS often involves both infections and autoimmune conditions and other immune system dysfunctions. Research is showing that deep tissue infections and bone and cartilage infections and nerve system infections are playing a key role in some autoimmune illnesses, including some forms of arthritis. These infections are difficult to diagnose and find and many patients remain undiagnosed and neglected. The immune system is attacking its own tissues, cells, cartilage, bone, nerves, etc. trying to get at viruses, bacteria, mycoplasma, pathogens, or in cases pathogens containing human tissue markers, with resultant inflammation and serious damage over time.Inflamed tissue / cartilage suggests an immune response to something, that something is usually a pathogen or in some cases a toxin. Analysis of the inflamed tissue informs the diagnosis. Analysis of the pathogen or toxin gives one the causative factor. ME/CFS is a disease of inflammation so finding inflammation is quite normal in the illness. The real challenge for medicine and science is to find the pathogen or toxin which initiates and perpetuates this chronic inflammatory immune response.
B-cells should be examined for infections (active and latent) involving viruses, lyme infections and co-infections, myocplasmas, bacteria, fungii, and for toxins. And tested for pathogens containing human tissue markers.
B cells with CD20 marker
(Important regarding drug Rituximab which was used many years later)
Klimas, N. G., F. R. Salvato, R. Morgan, and M. A. Fletcher. 1990. Immunologic abnormalities in chronic fatigue syndrome. J. Clin. Microbiol. 28:1403-1410.
Tirelli, U., A. Pinto, G. Marotta, M. Crovato, M. Quaia, P. De Paoli, E. Galligioni, and G. Santini. 1993. Clinical and immunologic study of 205 patients with chronic fatigue syndrome: a case series from Italy. Arch. Intern. Med. 153:116-117.
Rituximab trialsfor ME/CFS
Rituximab reduces or eliminates CD20+ B cells, reduces Th17 T cell production, reduces Il 2 levels and the production of NFκB.
Rituximab used in Multiple Scelorisisand Rheumatoid Arthritis
McFarland HF: The B cell-old player, new position on the team. N Engl J Med 2008, 2008:664-665
Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, Bar-Or A, Panzara M, Sarkar N, Agarwal S, Langer-Gould A, Smith CH, HERMES Trial Group: B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. New Engl J Med 2008, 358:676-68
Monson NL, Cravens PD, Frohman EM, Hawker K, Racke MK: Effect of rituximab on the peripheral blood and cerebrospinal fluid B cells in patients with primary progressive multiple sclerosis. Arch Neurol 2005, 62:258-264
Cross AH, Stark JL, Lauber J, Ramsbottom MJ, Lyons JA: Rituximab reduces B cells and T cells in cerebrospinal fluid of multiple sclerosis patients. J Neuroimmunol 2006, 180:63-70
Bar-Or A, Fawaz L, Fan B, Darlington PJ, Rieger A, Ghorayeb C, Calabresi PA, Waubant E, Hauser SL, Zhang J, Smith CH: Abnormal B-cell cytokine responses a trigger of T-cell-mediated disease in MS? Ann Neurol 2010, 67:452-461
Reichardt P, Dornbach B, Rong S, Beissert S, Gueler F, Loser K, Gunzer M: Naive B cells generate regulatory T cells in the presence of a mature immunologic synapse. Blood 2007, 110:1519-1529.
Emery P, Fleischmann R, Filipowicz-Sosnowska A, Schechtman J, Szczepanski L, Kavanaugh A, Racewicz AJ, van Vollenhoven RF, Li NF, Agarwal S, Hessey EW, Shaw TM, DANCER Study Group: The efficacy and safety of rituximab in patients with active rheumatoid arthritis despite methotrexate treatment: results of a phase IIB randomized, double-blind, placebo-controlled, dose-ranging trial. Arthritis Rheum 2006, 54:1390-1400
Eisenberg R: Update on rituximab. Ann Rheum Dis 2005, 64:iv55-iv57
Kappa/Lambda assay test
This is significant as kappa/lambda light chains are the result of abnormalities within the bone marrow B-cell lineage. In the book Osler's Web: Inside the Labyrinth of the Chronic Fatigue Syndrome Epidemic by Hillary Johnson medical doctors in the USA found an unusually high number of B cell lymphomas in ME patients. Special scientific tests showed that these B-cell Lymphomas in ME patients were unusual types, not seen before. The researchers found B-cell deficiency in all patients, and a positive result on the kappa/lambda assay for a majority of these patients. After studying samples from approximately fifty patients, Wormsley estimated that the rate of clonal excess abnormality in the CFS patients from Nevada was at least 25 percent ('Oslers Web, by Hillary Johnson, Penguin Books 1997, page 94). This is significant as kappa/lambda light chains are the result of abnormalities within the bone marrow B-cell lineage. This has direct on B-cells and overall immunity, and susceptibility to Cancers. Recent scientific studies show that the incidence rate of non-Hodgkin's lymphoma is 0.02% in the United States, yet nearly 5% of CFS patients develop the disease. This is a significant risk factor.
Gamma T cell clonal rearrangement Test
This tests for pre-Cancerous conditions related to ME . A certain percentage of ME patients are at high risk of getting B cell Lymphoma and other Cancers. This test is recommended by Dr. Dan Peterson who has been involved in treating ME pateints and in sceintific research since the early 1990's.
Naïve B cells are a high percentage of all B cells. Lowered levels of IL 21,12, and 27, which are involved in the maturation of B cells. These immature B-cells cannot properly target infections. Invest in ME Scientific Conference 2013 (Dr. Amolok Bansal).
Dr. Sonya Marshall-Gradisnik presented her research teams findings on NK cell and Immunological markers at the International ME Conference 2014. There is significant increase in naive B cell phenotypes, specifically memory and naive B cells, due to increased dendritic cell and cytokine production. This indicates an auto-immune response.
Bansal et al. found the following in ME patients in 2012 and 2013
' patients had greater numbers of naive B cells as a percentage of lymphocytes: 6·3 versus 3·9% in HC (P = 0·034), greater numbers of naive B cells as a percentage of B cells: 65 versus 47% in controls (P = 0·003), greater numbers of transitional B cells: 1·8 versus 0·8% in controls (P = 0·025) and reduced numbers of plasmablasts: 0·5 versus 0·9% in controls (P = 0·013). While the cause of these changes is unclear, we speculate whether they may suggest a subtle tendency to autoimmunity.'
Bansal et al., (2013), Altered functional B cell subset populations in patients with chronic fatigue syndrome compared to healthy controls. Clinical & Experimental Immunology, 172: 73–80.
7. Natural
Killer Cell Numbers and Function and Cytotoxicity Tests. Abnormal low numbers, poor function and low cytotoxic activity is the biomarker. (6). Natural killer numbers are usually 50% or more below normal, and lytic units and cytotoxic activity 50% or more below normal in ME patients.
Tests Genetic condition involving absence of NK cells in peripheral blood. This is a rare genetic condition involving three key genes (MCM4, FCGR3A, & GATA2) AbsoluteNatural Killer Cell count (ideally 200 or higher in healthy individuals) Natural Killer cell cytotoxicity tests
Natural Killer cell lysis tests
Natural Killer cell function tests NK cell signalling markers
NK cell
receptors tests - KIR receptors. NK cell
phenotypes tests CD56(dim) CD16(positive) CD56(bright) CD16(negative) Abnormal levels of Perforin, Lytic proteins, Granzyme A, B and Granzyme K expression Abnormal microRNA. Molecular level tests (mentioned in research papers below) Genetic polymorphisms that result in deficient NK cells
Excess of activating killer cell immunoglobulinlike receptors (KIRs) and lack of HLA-Bw4 ligands.
Increased levels of KIR3DS1 and a lack of KIR2DS5 with an absence of HLA-Bw4IIe80 on KIRS3DS1 and KIR3DL1
Pasi, A., Bozzini, S., Carlo-Stella, N., Martinetti, M., Bombardieri, S., De Silvestri, A., Salvaneschi, L. and Cuccia, M., 2011. Excess of activating killer cell immunoglobulinlike receptors and lack of HLA-Bw4 ligands: a twoedged weapon in chronic fatigue syndrome. Molecular medicine reports. 4, 535-40.
Dr. Sonya Marshall-Gradisnik presented her research teams findings on NK cell and Immunological markers at the International ME Conference 2014. They found a consistent decrease in NK lysis and the severity of the illness reflects the immune changes. There is significant loss of function in KIRs. The dim phenotype KIR2DL1 is significantly reduced, and CD94dim is increased in moderate and severe cases. Dendritic cells are increased significantly in moderate and severe cases. This is accompanied by increased production of cytokines, which cause clinical signs and symptoms. T cell phenotypes are significantly decreased with reduced lysis function. iNKT cells are increased in severe cases and this leads to increased cytokines. NK cell lysis is low and there is significant reduction in adhesion markers. There is decreased migratory ability of NK cells to migrate towards the antigen to lyse.
Reduced TRPM3 levels and intra cellular calcium levels and TRP
genetic abnormalitie which affect NK cell functions
"NK cytotoxic activity was significantly decreased in the CFS/ME patients at T1, T2 and T3 compared to the non-fatigued group. Additionally, in comparison to the non-fatigued controls, the CFS/ME group had significantly lower numbers of CD56 bright CD16 NK cells at both T1 and T2. Interestingly, following mitogenic stimulation, cytokine secretion revealed significant increases in IL-10, IFN-γ and TNF-α at T1 in the CFS/ME group. A significant decrease was observed at T2 in the CFS/ME group for IL-10 and IL-17A while at T3, IL-2 was increased in the CFS/ME group in comparison to the non-fatigued controls. Overall cytotoxic activity was significantly decreased at T3 compared to T1 and T2. CD56bright CD16 NK cells were much lower at T2 compared to T1 and T3. IL-10 and IL-17A secretion was elevated at T2 in comparison to T1 and T3"
"These results confirm decreases in immune function in CFS/ME patients, suggesting an increased susceptibility to viral and other infections. Furthermore, NK cytotoxic activity may be a suitable biomarker for diagnosing CFS/ME as it was consistently decreased during the course of the 12 months study." Longitudinal investigation of natural killer cells and cytokines in chronic fatigue syndrome/myalgic encephalomyelitis. Ekua W Brenu, Mieke L van Driel, Donald R Staines, Kevin J Ashton, Sharni L Hardcastle, James Keane, Lotti Tajouri, Daniel Peterson, Sandra B Ramos, and Sonya M Marshall-Gradisnik. J Transl Med. 2012; 10 : 88.
"Compared to healthy individuals, CFS/ME patients displayed significant increases in IL-10, IFN-γ, TNF-α, CD4+CD25+ T cells, FoxP3 and VPACR2 expression. Cytotoxic activity of NK and CD8+T cells and NK phenotypes, in particular the CD56bright NK cells were significantly decreased in CFS/ME patients. Additionally granzyme A and granzyme K expression were reduced while expression levels of perforin were significantly increased in the CFS/ME population relative to the control population. These data suggest significant dysregulation of the immune system in CFS/ME patients. Immunological abnormalities as potential biomarkers in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis Ekua W Brenu, Mieke L van Driel, Don R Staines, Kevin J Ashton, Sandra B Ramos, James Keane, Nancy G Klimas and Sonya M Marshall-Gradisnik. Journal of Translational Medicine 2011, 9:81
Abnormally high or low NKp46 and NKCD57 levels (subsets of patients and severity of condition is important)
" NK cells from CFS individuals displayed higher expression of NKp46 and CD69 but lower expression of CD25 in all NK subsets defined. Overall, T cell and NK cell features clearly clustered CFS individuals."
"A phenotypic feature of NK cells from CFS individuals is the low expression of CD57" Screening NK-, B- and T-cell phenotype and function in patients suffering from Chronic Fatigue Syndrome. Curriu et al. Journal of Translational Medicine 2013, 11:68
" lowest of NKCD57 and high or very high levels of NKp46 would be a severe clinical condition in CFS, in which the patient is bedridden, moves with difficulty even in a wheelchair, with visual and auditory nuisances important and that we wanted to be called "bed-couch."
Source: http://www.asssem.org/ (Spanish research body)
"low numbers of NKH1+T3- lymphocytes .................When tested for cytotoxicity against a variety of different target cells, patients with CFS consistently demonstrated low levels of killing."
73 percent of ME cases had a decrease in the number of NK cells, and the T3 negative subset was reduced in 50 percent.
Caligiuri
M, Murray C, Buchwald D, et al. Phenotypic and functional deficiency of natural killer cells in patients with chronic fatigue syndrome. J
Immunol 1987:139:3306-13.
Increased proportion of CD56+CD3+ T cells, which may explain decreased natural killer (NK) cell cytotoxic activity. Decreased percentage of CD56+Fcgamma receptor+ NK cells, which shows a reduced capacity for antibody-dependent cellular toxicity.
Caligiuri M, Murray C, Buchwald D, Levine H, Cheney P, Peterson D, Komaroff AL, Kitz J: Phenotypic and functional deficiency of natural killer cells in patients with chronic fatigue syndrome. J Immunol 139(10):3306-3313, 1987
Morrison LJ, Behan WH, Behan PO: Changes in natural killer cell phenotype in patients with post-viral fatigue syndrome. Clin Exp Immunol 83:441-446, 1991
This is a new way of identifying immune dysfunctions at the molecular level. Significant reductions in the expression levels of miR-21, in both the NK and CD8(+)T cells in the CFS/ME sufferers. Additionally, the expression of miR-17-5p, miR-10a, miR-103, miR-152, miR-146a, miR-106, miR-223 and miR-191 was significantly decreased in NK cells of CFS/ME patients in comparison to the non-fatigued controls. ( Cytotoxic lymphocyte microRNAs as prospective biomarkers for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Brenu EW, Ashton KJ, van Driel M, Staines DR, Peterson D, Atkinson GM, Marshall-Gradisnik SM. J Affect Disord. 2012 Dec 10;141(2-3):261-9.)
Decreases in several miRNAs - miR-1467a, miR-106b, miR-191, miR-223 increase production of pro-inflammatory molecules Immunology Primer for Practitioners.
Dr. Sonya Marshall-Gradisnik presented her research teams findings on Immunological markers at the International ME Conference 2014. MiRNA plasma in ME - significant differences are expressed between ME cases and non-fatigued controls.
Decrease in CD4+CD45+ T cells
Klimas N, Salvato F, Morgan R, Fletcher MA: Immunologic abnormalities in chronic fatigue syndrome. J Clin Microbiol 28(6):1403-1410, 1990
Studies from Japan where ME is called "Low natural killer cell syndrome". Low natural killer cell numbers and low level of cytotoxicity and function.
Aoki T, Miyakoshi H, and Usada Y et al: Low NK syndrome and its relationship to chronic fatigue syndrome. Clin Immunol Immunopathol. 69:253-65, 1993.
Aoki T, Usada Y, Miyakoshi H: A novel immunodeficiency: Low NK syndrome (LNKS). Jap J Med 3212:14-17, 1985
Aoki T, Usuda Y, Miyakashi H, et al: Low natural syndrome: clinical and immunologic features. Nat Immun Cell Growth Regul 6:116-128, 1987
Miyakoshi H, Aoki T, Mizukoshi: Acting mechanisms of Lentinan in humans. II. Enhancement of non-specific cell-mediated cytotoxicity as an interferon induced response. Int J Immunopharmacol 6:373-379, 1984
NK cell lysis is reduced. Significant reduction in Interferon-gamma in NK bright cells. CD107 degranulation- significant increase, suggesting impaired degranulation. Immunology Primer for Practitioners.
Natural Killer Cell Subset Distribution of Lytic Proteins in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis Teilah K. Huth, Ekua W. Brenu, Sharni L. Hardcastle, Kirsty Fuller, Sam Johnston, Donald R. Staines, Sonya M. Marshall-Gradisnik
Natural Killer Cell Degranulation in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis Teilah K. Huth, Ekua W. Brenu, Kirsty Fuller, Sharni L. Hardcastle, Sam Johnston, Donald R. Staines, Sonya M. Marshall-Gradisnik
Abnormal Perforin levels in Natural Killer cells and T-cells (CD8 cells). This adversely affects cytotoxic functions. (6)
Abnormalities in Granzyme A, B, and perforin are related to NK cell dysfunctions in ME
Natural Killer Cell Degranulation in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis
Teilah K. Huth, Ekua W. Brenu, Kirsty Fuller, Sharni L. Hardcastle, Sam Johnston, Donald R. Staines, Sonya M. Marshall-Gradisnik. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Nitrogen Balance deficiency. Essential for NK cells. (8)
Natural Killer Cell
Function and Cytotoxicity Tests - measured in
"Lytic" units expressed as
"LU" on Lab results. A low
level represents a seriously weakened
immune system and increased
susceptibility to viral, fungal or
bacterial illnesses
A very accurate NK Function test is
available through S.W. Immunotoxicology
Labs in Tucson, AZ. USA 602-451-6533. Ask for
Dr. Dean Friesen. He has developed a new
NK function test that is accurate to
within .2% upon retesting. NK Function
tests are also available from
ImmunoSciences Labs, USA (800-950-4686 or
310-657-1077) or Specialty Labs, USA
(800-421-7110 - test code 5420).
8(b) Pro-inflammatory TH2 cytokine dominance. Pro-inflammatory TH2 cytokine dominance in vast majority of patients. Profiling individual cytokines and trying to make them diagnostic for all patients cannot work due to
(i)
the existence of subgroups
(ii)
the progression of the illness over time in phases: 2 phases, one phase 3 years or less and one phase more than 3 years (Hornig et al. (2013, 2015). Immune system exhaustion can occur in those who are ill for 3 years or more.
(iii)
if the patient is having active infection(s) including opportunistic infections
(iv)
whether he/she is in remission or in relapse. And if they have mild, moderate or severe ME.
(v)
the patient's genetic weaknesses
(vi) gradual onset ME or rapid onset ?
.
Thus, differences have been found in individual cytokine markers between groups of patients. Using Pro-inflammatory TH2 cytokine dominance may provide an effective diagnostic tool.
Phase of illness related Cytokines
There are significant cytokine differences between patients who have the illness for 3 years or less and those who have it for 3 years or more. This is one of the most important findings in recent years. The p values in this research are less than 0.05 in many cases, with several less than 0.01, proving that several cytokines are playing an important role in the illness. Hornig et al.. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. 27 February 2015, Sci. Adv. 1, e1400121 (2015) DOI: 10.1126/sciadv.1400121 Click here to view scientific research papers and findings
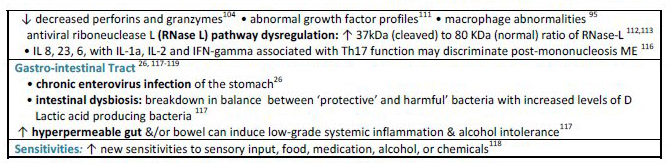
The following research compilation was presented by Dr. Dan Peterson at a Swedish ME/CFS conference in 2011. This test provides 94% accuracy according to some studies.
Levels of 51 inflammation-related molecules—cytokine family/chemoknes/hormones measured .
15 either distinguished cases from controls, or correlated with symptom severity, or both
Cytokine-by Cytokine Analyses of the Controls, Mild Cases (51-75). Moderate Cases (76-85) and Severe Cases (86-100) and matching this against symptom severity based on MF120. Adjusted for Matched Set
CCL11 - 0.00082
CD40L - 0.00067
CXCL1 - 0.00653
CXCL10 - 0.001-42
GM-CSF - 0.00108
IFN-7 - 0.00022
iL-5 - 0.00713
iL-7 - 0.00265
iL-12P70 - 0.00615
iL-13 - 0.00424
iL-17F - 0.00417
LEPTIN - 0.00402
LiF - 0.00702
RESISTIN - 5e-
Raised CCL11 and CXCL10, reduced CSF2, increased levels of Eotaxin (and decreased levels of IL1b) which show an allergic type reaction in the nervous system. These findings suggest an infection of the nervous system and abnormal microglia activation. A strong inflammatory TH2 cytokine response was found in ME patients.
Molecular Psychiatry. 2015 Mar 31. doi: 10.1038/mp.2015.29. [Epub ahead of print] Cytokine network analysis of cerebrospinal fluid in myalgic encephalomyelitis/chronic fatigue syndrome. Hornig M, Gottschalk G, Peterson DL, Knox KK, Schultz AF, Eddy ML, Che X, Lipkin WI
Innate Immune Changes in the
Peripheral Blood of Chronic Fatigue
Syndrome Patients: Risk Factors for
Disease Progression and Management
Deborah L. S. Goetz, Judy A. Mikovits
, Jamie Deckoff-Jones
and Francis W. Ruscetti,
LANDRES Management Consultant LLC 2
MAR Consulting Inc.
Private CFS Practice. Chronic Fatigue Syndrome. ISBN: 978-1-63321-961-8
GM-CSF
Stimulates proliferation of B and T lymphocytes and NK cells
Innate Immune Changes in the
Peripheral Blood of Chronic Fatigue
Syndrome Patients: Risk Factors for
Disease Progression and Management
Deborah L. S. Goetz, Judy A. Mikovits
, Jamie Deckoff-Jones
and Francis W. Ruscetti,
LANDRES Management Consultant LLC 2
MAR Consulting Inc.
Private CFS Practice. Chronic Fatigue Syndrome. ISBN: 978-1-63321-961-8
Innate Immune Changes in the
Peripheral Blood of Chronic Fatigue
Syndrome Patients: Risk Factors for
Disease Progression and Management
Deborah L. S. Goetz, Judy A. Mikovits
, Jamie Deckoff-Jones
and Francis W. Ruscetti,
LANDRES Management Consultant LLC 2
MAR Consulting Inc.
Private CFS Practice. Chronic Fatigue Syndrome. ISBN: 978-1-63321-961-8
also raised in Chalmydia infections
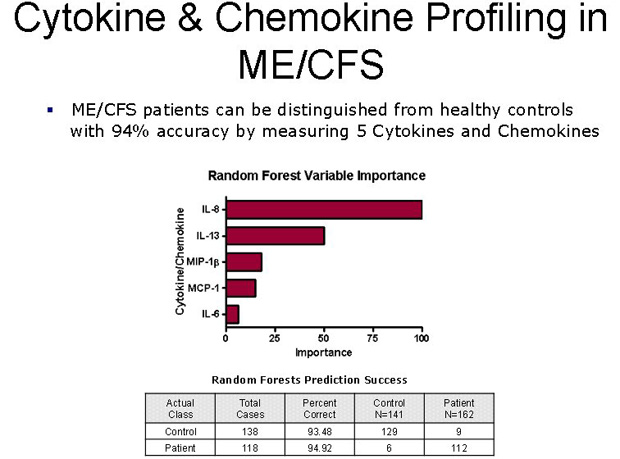
Cytokine co-expression networks
Cytokine co-expression networks were constructed from the pair-wise mutual information (MI) patterns found within each subject group. Networks for HC and CFS had visibly different topologies (geometric arrangements). A weighted spring-electrical embedding structurally reveals the subject-subject (inset) and cytokine-cytokine associations based on measurements in 59 healthy control subjects (A) and 40 CFS patients (B). All edge weights are significant at p≤0.01. Separation of subjects was consistent with their assignment to diagnostic groups supporting the use of within-group variation in the estimation of mutual information for cytokine-cytokine associations (73). Diagram used with permission.
Broderick G, Fuite J, Kreitz A, Vernonb SD, Klimas N, Fletcherd MA. A Formal Analysis of Cytokine Networks in Chronic Fatigue Syndrome. Brain Behav Immun 2010;24(7): 1209–1217. doi:10.1016/j.bbi.2010.04.012.
10. High level Immune tests & Neuro Inflammation tests which indicate infection(s) and/or immune system dysfunctions
(a) Test for Abnormal Nagalase levels which severely weaken immune system functions and indicate chronic infection. Nagalase can cause serious immune system dysfunction (7) (b) Test for activation and upregulation of Toll like receptors (TLR2/4)
(c) Test for the activation and upregulation of IL-1β,NF-kappaB, TNF-a, IL-6, IL-8, IL-10, IFNα, COX-2, IDO levels and pro inflammatory cytokines, activation of microglia and astrocytes, inflammatory markers and oxidative and nitrosative stress. Also test for astrocyte abnormalities such as reduced numbers and function. (d) Test for high Glutamate levels and quinolinic acid levels in the brain and nervous system (e) Test for peripheral immune activation and neuroinflammation using FLAIR magnetic resonance imaging (MRI) (f) Check for Lymphadenopathy and Lymphocytosis. This will require physical examinations and a few tests and if necessary a biopsy of inflamed or swollen tissues. Also check for tenderness
on
palpation
of
enlarged
lymph
glands
and
over
the
liver and spleen. Check for morphological
changes
in
the
lymphocytes
with
relative
lymphocytosis
and
eosinophilia.
"In about half
the cases, relative lymphocytosis was seen
during the early course of the illness"
"Similar findings have been reported in the
endemic cases in the neighborhood of the
Royal Free Hospital"
"A
relative lymphocytosis wa
s also observed in
one-third of the Bethesda cases. The small
Berlin outbreak differed in that a
polymorphonuclear leukocytosis occurred in all
seven patients" The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromyasthenia. Dr. Acheson, American Journal of Medicine, 1959.
11. Genes coding for immune system, microbe infections, inflammatory system, cell apoptosis and oxidative stress
12. T-cell abnormalities. Abnormally CD4/CD8 ratio, Low CD8 numbers, function and cytotoxicity. T reg cell abnormalities.CD8 and cytotoxic T cells bearing activation antigens CD38 and HLA-DR.
Abnormally High or Low CD4/CD8 ratio found in subsets of patients
- "Patients had a higher mean (+/- SD) CD4/CD8 T-cell ratio than matched healthy controls (3.16 +/- 1.5 compared with 2.3 +/- 1.0, respectively; P < 0.003)."
Buchwald, D., Cheney, P., Peterson, D., Henry, B., Wormsley, S., Geiger, A., Ablashi, D., Komaroff, D.etc. 1992. A chronic illness characterized by fatigue, neurologic and immunologic disorders, and active Human Herpesvirus Type 6 Infection. Annals of Internal Medicine 1116: 103-13. (The seminal scientific research paper on the Lake Tahoe epidemic in the USA in the mid 1980's and the origin of the term CFS).
- Get CD4 and CD8 cell counts. Normal ratio for CD4 cell : CD8 cell is 2 or 3. Test for abnormal ratio which suggests immune dysfunction.
Abnormal Low CD4/CD8 ratio found
in some studies
- Klimas, N. G., F. R. Salvato, R. Morgan, and M. A. Fletcher. 1990. Immunologic abnormalities in chronic fatigue syndrome. J. Clin. Microbiol. 28:1403-1410
- Levine, P. H., T. L. Whiteside, D. Friberg, J. Bryant, G. Colclough, and R. B. Herberman. 1998. Dysfunction of natural killer activity in a family with chronic fatigue syndrome. Clin. Immunol. Immunopathol. 88:96-104.
- Straus, S. E., S. Fritz, J. K. Dale, B. Gould, and W. Strober. 1993. Lymphocyte phenotype and function in the chronic fatigue syndrome. J. Clin. Immunol. 13:30-40.
CD45RO increased
- Straus, S. E., S. Fritz, J. K. Dale, B. Gould, and W. Strober. 1993. Lymphocyte phenotype and function in the chronic fatigue syndrome. J. Clin. Immunol. 13:30-40.
A reduced CD8 suppressor cell population and increased activation markers (CD38, HLA-DR) on CD8 cells were found.
- Landay, A. L., C. Jessop, E. T. Lennette, and J. A. Levy. 1991. Chronic fatigue syndrome: clinical condition associated with immune activation. Lancet 338:707-712.
- Klimas, N. G., F. R. Salvato, R. Morgan, and M. A. Fletcher. 1990. Immunologic abnormalities in chronic fatigue syndrome. J. Clin. Microbiol. 28:1403-1410.
- Lloyd, A. R., D. Wakefield, C. R. Boughton, and J. M. Dwyer. 1989. Immunological abnormalities in the chronic fatigue syndrome. Med. J. Austral. 151:122-124
Regulatory T cells (Treg)
- "A significant increase in Tregs was observed in both 1994 CDC
and ICC patients in comparison to healthy controls (Figure 2). Further,
a significant decrease in CD39
+
Tregs was observed in 1994 CDC
patients in comparison to healthy controls............ HNA2 (CD177
-
) were significantly increased in 1994 CDC patients while HNA2
(CD177
+
) were significantly reduced in ICC patients in comparison to
healthy controls (Figure 3). HNA5 was higher in 1994 CDC patients in
comparison to ICC patients."
Brenu et al.. Immune Abnormalities in Patients Meeting New Diagnostic Criteria for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis.J Mol Biomark Diagn 2013, 4:3
- T-cell subsets and phenotypes. "CFS diagnosed individuals showed similar absolute numbers of T, B and NK cells, with minor differences in the percentage of CD4+ and CD8+ T cells. B cells showed similar subset frequencies and proliferative responses between groups. Conversely, significant differences were observed in T cell subsets. CFS individuals showed increased levels of T regulatory cells (CD25+/FOXP3+) CD4 T cells, and lower proliferative responses in vitro and in vivo. Moreover, CD8 T cells from the CFS group showed significantly lower activation and frequency of effector memory cells. No clear signs of T-cell immunosenescence were observed."
"increase in the proportion of CD4 T-cells expressing the PD-1 (CD279) marker"
"CD8 T-cells expressing the CD5 marker were higher"
"lower counts of the activation marker CD38 and memory CD8 T-cells displaying the marker CD45RO." Screening NK-, B- and T-cell phenotype and function in patients suffering from Chronic Fatigue Syndrome. Curriu et al. Journal of Translational Medicine 2013, 11:68
- Raised levels of proinflammatory cytokines, increased levels of interleukin IL 1 and tumor necrosis factor-α, nuclear factor κB, Increased cyclo-oxygenase 2, IL 2, IL 10, transforming growth factor β, osteopontin levels, neopterin, T regulatory (Treg) dysfunction, Forkhead box P3 (FOXP3) dysfunction, Clonal exhaustion of T cells, raised CD26, CD69 expression, activation of immunoinflammatory pathways.
Gerwyn Morris and Michael Maes. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. Morris and Maes BMC Medicine 2013 11:205 doi:10.1186/1741-7015-11-205.
- Chronic IL 2 and the exhaustion of FOXP3 expression on CD25 + CD4+ Treg cells over time
Ziegler SF, Buckner JH: FOXP3 and the regulation of Treg/Th17 differentiation. Microbes Infect 2009, 11:594-598.
- Increases in CD4(+)CD25(+) Treg cells and FOXP3 expression. Liu DH, Liu ZD, Li YZ, Zhang HY, Hu CJ, Zhang YB, Whang DX: Expression of lymphocyte subsets and CD25 ~ + regulative T Cells in peripheral blood of patients with chronic fatigue syndrome. Labeled Immunoassays and Clinical Medicine. Abstract 2011, 2011–02.
miRna and Molecular level tests
-
This is a new way of identifying immune dysfunctions at the molecular level. Significant reductions in the expression levels of miR-21, in both the NK and CD8(+)T cells in the CFS/ME sufferers. Additionally, the expression of miR-17-5p, miR-10a, miR-103, miR-152, miR-146a, miR-106, miR-223 and miR-191 was significantly decreased in NK cells of CFS/ME patients in comparison to the non-fatigued controls. ( Cytotoxic lymphocyte microRNAs as prospective biomarkers for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Brenu EW, Ashton KJ, van Driel M, Staines DR, Peterson D, Atkinson GM, Marshall-Gradisnik SM. J Affect Disord. 2012 Dec 10;141(2-3):261-9.)
-
mRNA CD8 cells show consistent abnormalities (Invest in ME Scientific Conference, 2012, 2013, Dr. Donald Staines)
-
Dr. Sonya Marshall-Gradisnik presented her research teams findings on Immunological markers at the International ME Conference 2014. MiRNA plasma in ME - significant differences are expressed between ME cases and non-fatigued controls.
Reduced Granzyme A and Granzyme K expression
- "Compared to healthy individuals, CFS/ME patients displayed significant increases in IL-10, IFN-γ, TNF-α, CD4+CD25+ T cells, FoxP3 and VPACR2 expression. Cytotoxic activity of NK and CD8+T cells and NK phenotypes, in particular the CD56bright NK cells were significantly decreased in CFS/ME patients. Additionally granzyme A and granzyme K expression were reduced while expression levels of perforin were significantly increased in the CFS/ME population relative to the control population. These data suggest significant dysregulation of the immune system in CFS/ME patients."
- Immunological abnormalities as potential biomarkers in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Ekua W Brenu, Mieke L van Driel, Don R Staines, Kevin J Ashton, - Sandra B Ramos, James Keane, Nancy G Klimas, Sonya M Marshall-Gradisnik. Journal of Translational Medicine 2011, 9:81. (2011) - Abnormalities in Granzyme A, B, and perforin are related to NK cell dysfunctions in ME
Natural Killer Cell Degranulation in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis
Teilah K. Huth, Ekua W. Brenu, Kirsty Fuller, Sharni L. Hardcastle, Sam Johnston, Donald R. Staines, Sonya M. Marshall-Gradisnik. IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Elevated CD26 levels
- "Percent CD2+ lymphocytes (T cells and NK cells) positive for DPPIV/C26 was elevated in CFS cases, but there was a decrease in the number of molecules (rMol) of DPPIV/C26 expressed on T cells and NK cells and a decrease in the soluble form of the enzyme in serum." ( Biomarkers in Chronic Fatigue Syndrome: Evaluation of Natural Killer Cell Function and Dipeptidyl Peptidase IV/CD26 Mary A. Fletcher et al. PLoS One. 2010 )
- Raised levels of proinflammatory cytokines, increased levels of interleukin IL 1 and tumor necrosis factor- α, nuclear factor κB, Increased cyclo-oxygenase 2, IL 2, IL 10, transforming growth factor β, osteopontin levels, neopterin, T regulatory (Treg) dysfunction, Forkhead box P3 (FOXP3) dysfunction, Clonal exhaustion of T cells, raised CD26, CD69 expression, activation of immunoinflammatory pathways.
Gerwyn Morris and Michael Maes. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. Morris and Maes BMC Medicine 2013 11:205 doi:10.1186/1741-7015-11-205.
- Review: Immunology of Chronic Fatigue Syndrome Roberto Patarca, Timothy Mark, Mary Ann Fletcher and Nancy Klimas
CD69 marker.
- "The expression of the CD69 activation marker on T cells (CD3+, CD3+CD4+, and CD3+CD8+) and on NK cells (CD45+CD56+) was significantly lower in CFS patients than in healthy subjects. These differences were significant to the extent that a significant diagnostic performance was obtained, i.e. the area under the ROC curve was around 89%. No differences either in the number of leukocytes or in the number or percentage of lymphocytes, i.e. CD3, CD4, CD8 and CD19, could be found between CFS patients and the controls. Patients with CFS show defects in T- and NK cell activation." Decreased expression of CD69 in chronic fatigue syndrome in relation to inflammatory markers: evidence for a severe disorder in the early activation of T lymphocytes and natural killer cells. Mihaylova I, DeRuyter M, Rummens JL, Bosmans E, Maes M.. Neuro Endocrinol Lett. 2007 Aug;28(4):477-83.
- Raised levels of proinflammatory cytokines, increased levels of interleukin IL 1 and tumor necrosis factor-α, nuclear factor κB, Increased cyclo-oxygenase 2, IL 2, IL 10, transforming growth factor β, osteopontin levels, neopterin, T regulatory (Treg) dysfunction, Forkhead box P3 (FOXP3) dysfunction, Clonal exhaustion of T cells, raised CD26, CD69 expression, activation of immunoinflammatory pathways.
Gerwyn Morris and Michael Maes. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. Morris and Maes BMC Medicine 2013 11:205 doi:10.1186/1741-7015-11-205.
Clonal exhaustion of T cells
- Raised levels of proinflammatory cytokines, increased levels of interleukin IL 1 and tumor necrosis factor-α, nuclear factor κB, Increased cyclo-oxygenase 2, IL 2, IL 10, transforming growth factor β, osteopontin levels, neopterin, T regulatory (Treg) dysfunction, Forkhead box P3 (FOXP3) dysfunction, Clonal exhaustion of T cells, raised CD26, CD69 expression, activation of immunoinflammatory pathways.
Gerwyn Morris and Michael Maes. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. Morris and Maes BMC Medicine 2013 11:205 doi:10.1186/1741-7015-11-205.
A reduced CD8 suppressor cell population and increased CD8+ T-cells bearing activation antigens (CD38+ , HLA-DR). This has been found in a few studies (4,6)
- T-cell subsets and phenotypes. "CFS diagnosed individuals showed similar absolute numbers of T, B and NK cells, with minor differences in the percentage of CD4+ and CD8+ T cells. B cells showed similar subset frequencies and proliferative responses between groups. Conversely, significant differences were observed in T cell subsets. CFS individuals showed increased levels of T regulatory cells (CD25+/FOXP3+) CD4 T cells, and lower proliferative responses in vitro and in vivo. Moreover, CD8 T cells from the CFS group showed significantly lower activation and frequency of effector memory cells. No clear signs of T-cell immunosenescence were observed."
- "increase in the proportion of CD4 T-cells expressing the PD-1 (CD279) marker"
- "CD8 T-cells expressing the CD5 marker were higher"
- "lower counts of the activation marker CD38 and memory CD8 T-cells displaying the marker CD45RO." Screening NK-, B- and T-cell phenotype and function in patients suffering from Chronic Fatigue Syndrome. Curriu et al. Journal of Translational Medicine 2013, 11:68
- "Compared to healthy individuals, CFS/ME patients displayed significant increases in IL-10, IFN-γ, TNF-α, CD4+CD25+ T cells, FoxP3 and VPACR2 expression. Cytotoxic activity of NK and CD8+T cells and NK phenotypes, in particular the CD56bright NK cells were significantly decreased in CFS/ME patients. Additionally granzyme A and granzyme K expression were reduced while expression levels of perforin were significantly increased in the CFS/ME population relative to the control population. These data suggest significant dysregulation of the immune system in CFS/ME patients. Immunological abnormalities as potential biomarkers in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis Ekua W Brenu, Mieke L van Driel, Don R Staines, Kevin J Ashton, Sandra B Ramos, James Keane, Nancy G Klimas and Sonya M Marshall-Gradisnik. Journal of Translational Medicine 2011, 9:81
-
CD8 lysis reduced and high levels of HNA2 (Invest in ME Scientific Conference, 2012, 2013, Dr. Donald Staines)
- Lymphopenia in a subset of patients (Invest in ME Scientific Conference, 2013 Professor Carmen Scheibenbogen, Berlin,Germany)
- Reduced cytotoxic activity of CD8+ T cells and NK phenotypes, in particular the CD56 bright NK cells (4,6)
- Cytotoxic T-cells (CD8+ T-cells) deficiency. This can predispose a person to infection and autoimmunity (Pender).
- Polyclonal immunoglobulin was elevated in 25% of patients and there was evidence for immunodeficiency in a further 25%. There was MBL deficiency in 15% (and 7% in controls) making these patients more prone to infection.
(Invest in ME Scientific Conference, 2013 Professor Carmen Scheibenbogen, Berlin,Germany)
- Abnormal Perforin Levels in Natural Killer cells and T-cells (CD8 cells) (6)
Decreased CD3 on lymphocytes
-
Subira ML, Castilla A, Civeira MP, et al: Deficient display of CD3 on lymphocytes of patients with chronic fatigue syndrome. J Infect Dis 160:165-166, 1989
13. Immunoglobulins
Abnormally low levels of IgG1, 2 and 3 in subgroups
Reduced IgG subclass 1 and 3. This suggests infection and lowered ability to fight active infections and control latent infections.
IgG, Immune complex, and Atypical Lymphocyte count abnormalities. Bates DW et al. Arch Intern Med 1995; 155: 97. (10 year study).
IgM-related immune response directed against neopitopes.
Maes M, Mihaylova I, Leunis JC: Chronic fatigue syndrome is accompanied by an IgM-related immune response directed against neopitopes formed by oxidative or nitrosative damage to lipids and proteins. Neuro Endocrinol Lett 2006, 27:615-621
Polyclonal immunoglobulin was elevated in 25% of patients and there was evidence for immunodeficiency in a further 25%. There was MBL deficiency in 15% (and 7% in controls) making these patients more prone to infection.
(Invest in ME Scientific Conference, 2013 Professor Carmen Scheibenbogen, Berlin,Germany)
Patarca, R. (2001), Cytokines and Chronic Fatigue Syndrome. Annals of the New York Academy of Sciences, 933: 185–200. doi: 10.1111/j.1749-6632.2001.tb05824.x
Wakefield, D., A. Lloyd, and A. Brockman. 1990. Immunoglobulin subclass abnormalities in patients with chronic fatigue syndrome. Pediatr. Infect. Dis. J. 9(Suppl.):S50-S53.
Lloyd, A. R., D. Wakefield, C. R. Boughton, and J. M. Dwyer. 1989. Immunological abnormalities in the chronic fatigue syndrome. Med. J. Austral. 151:122-124.
Natelson, B. H., J. J. LaManca, T. Denny, A. C. Vladutiu, J. Oleske, M. Hill, M. T. Bergen, L. Korn, and J. Hay. 1998. Immunological parameters in chronic fatigue syndrome, major depression, and multiple sclerosis. Am. J. Med. 105:43S-49S.
14. Lymphocytosis (major lymphocyte subsets: T cells, B cells and NK cells)
This is found in 20% of patients according to Dr. De Meirleir ( Chronic Fatigue Syndrome: A Biological Approach By Patrick Englebienne and Dr. Kenny De Meirleir ) and some other studies (Mitterer, M; Pescosta et al (July 1995). "Chronic active Epstein-Barr virus disease in a case of persistent polyclonal B-cell lymphocytosis". Br J Haematol 90 (3): 526–31.)
This typically indicates infection and/or reactivated latent pathogens.
15. Clonal TCR
?
Rearrangement
Testing
Used by Dr. Dan Peterson.
T cells
play active role in regulation and resolution of pathogen induced immune responses. They
accumulate at sites of inflammation and are closely associated with Viral, Parasitic and bacterial Infections. Also
associated with autoimmune diseases. They
upregulate MIP1
a
,
TNF
a
,
IL-10, IFN
n
Tests suggest chronic active infection particularly CMV.
Predictive of lymphoma development
Clinical Criteria for Testing
-
Acute (viral) onset ME/CFS
and/or
Lymphadenopathy and/or splenomega
16. Other Immune Markers
Serpin
Upregulation of Serpin in ME patients. This is important in the context of viral infection, immune dysfunction, RnaseL abnormality and elastase activity (Findings of Hornig et al., September 2013).
Elevated levels of Immune Complexes
Straus SE, Tosato G, Armstrong G, et al: Persisting illness and fatigue in adults with evidence of Epstein-Barr virus infection. Ann Intern Med 102:7-16, 1985
Borysiewicz LK, Haworth SJ, Cohen J, et al: Epstein-Barr virus - specific immune defects in patients with persistent symptoms following infectious mononucleosis. Q J Med 58:111-121, 1986
Behan PO, Behan WHM, Bell EJ: The postviral fatigue syndrome - An analysis of the findings in 50 cases. J Infect 1985;10:211-22, 1985
Bates DW, Buchwald D, Lee J, Kith P, Doolittle T, Rutherford C, Churchill WH, Schur PH, Werner M, Wybenga D, et al: Clinical laboratory test findings in patients with chronic fatigue syndrome. Arch of Intern Med 155:97-103, 1995
Elevated Eosinophil levels in ME patients who have illness for 3 years or less. ( findings of Hornig et al., September 2013)
Also other studies show elevated serum levels of Eosinophil Cationic Protein (ECP). RAST positivity to one or more allergens was 77%.
Conti F, Magrini L, Priori R, Valesini G, Bonini S: Eosinophil cationic protein serum levels and allergy in chronic fatigue syndrome. Allergy 51(2):124-127, 1996
Abnormal Lysozyme levels. Elevated Serum IL-1, TNFα, neopterin and lysozyme levels. "Serum IL-1, TNFα, neopterin and lysozyme are significantly higher in patients with ME/CFS than in controls" ( Evidence for inflammation and activation of cell-mediated immunity in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Increased interleukin-1, tumor necrosis factor-α, PMN-elastase, lysozyme and neopterin. Michael Maes et al. Journal of Affective Disorders Volume 136, Issue 3, February 2012, Pages 933–939 )
IgM-related immune response directed against neopitopes formed by oxidative or nitrosative damage to lipids and proteins
Maes M, Mihaylova I, Leunis JC: Chronic fatigue syndrome is accompanied by an IgM-related immune response directed against neopitopes formed by oxidative or nitrosative damage to lipids and proteins. Neuro Endocrinol Lett 2006, 27:615-621.
Increased apoptosis of immune cells. And enhanced mRNA and protein levels of the IFN-induced protein kinase RNA (PKR). Vojdani A, Ghoneum M, Choppa PC, Magtoto L, Lapp CW: Elevated apoptotic cell population in patients with chronic fatigue syndrome: The pivotal role of protein kinase RNA. Journal of Internal Medicine 242(6):465-478, 1997
Antibody to the muscle tissue in the arterial bed. It is elevated in about 5% of M.E. patients. Dr. Byron Hyde Immune system Diagnostic Tests
Decrease in neutrophil respiratory bursts. Neutrophil antigens HNA-2 and HNA-5 are abnormal. Invest in ME Scientific Conference, 2012, 2013 (Dr. Donald Staines)
General Inflammation Markers:
high-sensitivity c-reactive protein (hs-CRP), white blood cell count (WBC) , IL-6. prostaglandins E2 and C3A . (Psychoneuroendocrinology 2008:33:18-29)
Erythrocyte sedimentation rate and C reactive protein levels and C3 complement activation
Defective Cell Mediated Immunity. MultiTest CMI Test (Cell
Mediated Immunity). Cell Mediated Immunity is reduced or ineffective. Tests general immune
system functioning. A Multitest CMI is
manufactured by Connaught Laboratories,
Route 611, Box 187, Swiftwater, PA 18370
Ph No 717-839-5467 or 800-822-2463 Fax
717-839-5005. (6)
DNCB Test - to measure immune
responsiveness. To order a Starter Kit,
contact DNCB Treatment Group, 2261
Market St, #436, San Francisco, CA 94114. Instructions come with the Kit. Read them
thoroughly before using the product
High
levels of quinolinic acid, a serious neurotoxin. Found in infectious diseases.
A very accurate NK Function test is
available through S.W. Immunotoxicology
Labs in Tucson, AZ. USA 602-451-6533. Ask for
Dr. Dean Friesen. He has developed a new
NK function test that is accurate to
within .2% upon retesting. NK Function
tests are also available from
ImmunoSciences Labs, USA (800-950-4686 or
310-657-1077) or Specialty Labs, USA
(800-421-7110 - test code 5420).
MultiTest CMITest (Cell
Mediated Immunity). Cell Mediated Immunity is reduced or ineffective. Tests general immune
system functioning. A Multitest CMI is
manufactured by Connaught Laboratories,
Route 611, Box 187, Swiftwater, PA 18370
Ph No 717-839-5467 or 800-822-2463 Fax
717-839-5005. (6)
Check reputable private Laboratories can be identified on the Internet
17.Vaccines - test for Adverse Immune System reactions to some vaccines
Kerr et al provide evidence of other triggers of (ME)CFS which include Parvovirus; C. pneumoniae; C. burnetti; toxin exposure and vaccination including MMR, pneumovax, influenza, hepatitis B, tetanus, typhoid and poliovirus (LD Devanur, JR Kerr. Journal of Clinical Virology 2006: 37(3):139-150).
Some individuals and subgroups develop adverse immune system reactions to vaccines. This is related to one's genes, and genetic structure including weaknesses and predispositions (for certain illnesses). Other factors include status and strength of one's immune system prior to vaccination, mercury in vaccines, aluminium in vaccines, adjuvants in vaccines and other types of vaccine contamination involving pathogens, toxins, and chemicals. Also the number of vaccines given at once and the age of the person is important. The immune system can be overwhelmed by multiple vaccinations in a short period of time. Additionally, the immune systems of children are not fully developed, and are thus vulnerable. These issues are often overlooked by medical doctors, yet they are a significant factor in immune system illnesses and degenerative illness. Several high profile court cases and compensation payments to patients show that this is a serious medical problem.
18. Tests for Autoimmune Disorders including autoimmune marker mimcry by viruses
It is worth noting that relatively high proportions of HLA-DR+ T cells have been reported in a number of autoimmune disorders.
Research is showing that deep tissue infections and bone and cartilage infections and nerve system infections are playing a key role in some autoimmune illnesses, including some forms of arthritis. These infections are difficult to diagnose and find and many patients remain undiagnosed and neglected. The immune system is attacking its own tissues, cells, cartilage, bone, nerves, etc. trying to get at viruses, bacteria, Lyme, mycoplasma, pathogens, or in some cases pathogens containing human tissue markers, with resultant inflammation and serious damage over time.Inflamed tissue / cartilage suggests an immune response to something, that something is usually a pathogen or in some cases a toxin. Analysis of the inflamed tissue informs the diagnosis. Analysis of the pathogen or toxin gives one the causative factor. ME/CFS is a disease of inflammation so finding inflammation is quite normal in the illness. The real challenge for medicine and science is to find the pathogen or toxin which initiates and perpetuates this chronic inflammatory immune response.
Inflamed tissue, cartilage and cells should be examined for infections (active and latent) and auto-antibodies and autoimmune markers. And tested for pathogens containing integrated cell human tissue markers.
Cytotoxic T-cells (CD8+ T-cells) deficiency. This can predispose a person to infection and autoimmunity (Pender).
Anticardiolipin Antibodies Test
Research recently shows the IgM isotype of ACA was present in 95% of CFS patients tested (2) This is an unusually high percentage and is an important finding. It suggests autoimmunity as anticardiolipin antibodies have consistently been found in autoimmune diseases and some infectious diseases. This may correlate to B-cell abnormalities in ME and the effectiveness of the drug Rituximab in clinical investigations, which is used for autoimmune conditions.
The enzyme-linked immunoassay (ELISA) method can be performed according to the instructions from the commercial ELISA kit to quantify IgA, IgG, and IgM ACA (QUANTA Lite ACA Anticardiolipin Kit, INOVA Diagnostics Inc., San Diego, CA). Test for IgM isotype of ACA.
Test for IgM isotype of ACA. This could be undertaken in a major hospital under the supervision of an Immunologist
Tests for Anti lamin antibodies
There is evidence of Antilamin antibodies in many ME patients (Findings of Dr. Malcolm Hooper. Anti-nuclear envelope antibodies: Clinical associations. Semin Arthritis Rheum 2001 Apr;30(5):313-320 Nesher G, Margalit R, Ashkenazi YJ.). This test can be carried out in a major hospital.
Autoantibodies to insoluble cellular antigens (vimentin and lamin B1, and a nuclear matrix antigen that colocalizes with a group of proteins involved in pre-mRNA splicing)
"Three major antigen-antibody systems in CFS have been characterized. Most patients with CFS have autoantibodies to the nuclear envelope protein lamin B1, the cytoskeletal protein vimentin, and a nuclear matrix antigen that colocalizes with a group of proteins involved in pre-mRNA splicing. Our studies on these autoantibodies are being done in collaboration with investigators at the University of Washington in Seattle and at Harvard University. We are developing a quantitative assay for serologic markers that may help to distinguish patients with CFS from persons without CFS and from patients with other diseases with features of chronic fatigue."
Source: http://www.scripps.edu/news/scientificreports/sr97/MEM97.html (Scripps Institute)
von Mikecz A, Konstantinov K, Buchwald DS, Gerace L, Tan EM: High frequency of autoantibodies in patients with chronic fatigue syndrome. Arthritis & Rheumatism 40(2):295-305, 1997
Autoantibodies to nuclear envelope antigens in chronic fatigue syndrome.
K Konstantinov, A von Mikecz, D Buchwald, J Jones, L Gerace, and E M Tan. J Clin Invest. Oct 15, 1996; 98(8): 1888–1896.
Antinuclear antibodies and other autoimmune factors
"25% developed varying autosoma
l antibodies of which,
for instance, antithyroid antibodies were found in
20% of cases studied." Myalgic Encephalomyelitis: Guidelines for Doctors John Richardson. Journal: J of Chronic Fatigue Syndrome, Vol. 10(1)
2002, pp. 65-80.
Anti-neuronal antibody Test
Buchwald MD, Wener MH, Komaroff AL: Antineuronal antibody levels in chronic fatigue syndrome patients with neurologic abnormalities. Arthritis Rheum 1991, 34:1485-1486.
Bates, D. W., D. Buchwald, J. Lee, P. Kith, T. Doolittle, C. Rutherford, W. H. Churchill, P. H. Schur, M. Wener, D. Wybenga, J. Winkelman, and A. L. Komaroff. 1995. Clinical laboratory test findings in patients with chronic fatigue syndrome. Arch. Intern. Med. 155:97-103.
Konstantinov, K., A. Von Mikecz, D. Buchwald, J. Jones, L. Gerace, and E. M. Tan. 1996. Autoantibodies to nuclear envelope antigens in chronic fatigue syndrome. J. Clin. Investig. 98:1888-1896.
Nishikai, M., S. Tomomatsu, R. W. Hankins, S. Takagi, K. Miyachi, S. Kosaka, and
K. Akiya. 2001. Autoantibodies to a 68/48 kDa protein in chronic fatigue syndrome and primary fibromyalgia: a possible marker for hypersomnia and cognitive disorders. Rheumatology 40:806-810.
Abnormal Leptin levels are found in several autoimmune illnesses such as autoimmune diabetes, autoimmune thyroid disorders, MS, rheumatoid arthritis and Lupus.
Tests for molecular mimicry
New research by Knox et al. suggests that the viruses consistently found in ME share molecular homologies for autoimmune disease markers of the thyroid, lupus, MS. These viruses may be invovled in molecular mimicry of some autoimmune markers (3). This may be leading to the autoimmune disorders found in ME , and to the effectiveness of Rituximab an autoimmune drug. This is fascinating as ME patients have many of the neurological symptoms found in autoimmune illnesses and MS. These autoimmunity tests are being developed for ME.
Abnormal levels of HLA-DQ3 (Keller et al, 1992)
19. Test for Protein M
Bacteria
have evolved to use a protein called 'Protein M' to block all antibodies produced by the human immune system. This remarkable discovery by scientists at the Scripps Research Institute in 2014 sheds new light on chronic bacteria infections in humans. As many ME patients have chronic infections, this information is important. Tests are being developed for Protein M. See paper below
- http://www.scripps.edu/news/press/2014/20140206lerner.html
22. Test for Vitamin D deficiency and B-12 deficiency
Vitamin D is essential for immune system health and many people living in northern latitude countries are deficient. The Vitamin D test can be carried out in a major hospital or in private laboratories.
Vitamin B-12 deficiency is common in ME and CFS patients.
23. Test for Intestinal bacteria associated with normal Immune system functions
Several strains of Intestinal bacteria are involved in regulating the immune system. Too much bad bacteria and parasites can adversely affect the immune system, causing dysfunction and dysregulation. This is the subject of ongoing scientific research worldwide.
For tests, see Section Intestinal toxic damage with effects on the immune system, mitochondria, glands and nervous system
23. Other Immune Dysfunction tests
Lymphocyte microRNAs Test
This is a new way of identifying immune dysfunctions at the molecular level. Significant reductions in the expression levels of miR-21, in both the NK and CD8(+)T cells in the CFS/ME sufferers. Additionally, the expression of miR-17-5p, miR-10a, miR-103, miR-152, miR-146a, miR-106, miR-223 and miR-191 was significantly decreased in NK cells of CFS/ME patients in comparison to the non-fatigued controls. ( Cytotoxic lymphocyte microRNAs as prospective biomarkers for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Brenu EW, Ashton KJ, van Driel M, Staines DR, Peterson D, Atkinson GM, Marshall-Gradisnik SM. J Affect Disord. 2012 Dec 10;141(2-3):261-9.)
Idiopathic CD4+ T lymphocytopeniaor non HIV AIDS
There are many similarities between ME and Idiopathic CD4+ T lymphocytopenia. They are so similar that some people believe they are the same illness. Idiopathic CD4+ T lymphocytopenia has also been called non-HIV AIDS, which means it is an immune system deficiency and dysfunction without the HIV virus. The involvement of other viruses and toxins have been proposed in this illness. Click here to view some scientific studies into this illness. Further scientific research will be required to establish if they are the same illness or if Idiopathic CD4+ T lymphocytopenia is a subgroup of ME or if they are different illnesses which are similar in some respects. This is important in the context of causative factors, structure of causation and the perpetuating factors in the illness.
There are tests for Idiopathic CD4+ T lymphocytopenia or non hiv aids as it is also called
2. Anticardiolipin Antibodies in the Sera of Patients with Diagnosed Chronic Fatigue Syndrome Yoshitsugi Hokama, Cara Empey Campora, Cynthia Hara, Tina Kuribayashi, Diana Le Huynh, and Kenichi Yabusaki. Department of Pathology, John A. Burns School of Medicine, University of Hawaii at Maˆnoa, Honolulu, Hawaii. Journal of Clinical Laboratory Analysis 23 : 210–212 (2009).
3. Knox, K., et al. Systemic Leukotropic Herpesvirus Infections and Autoantibodies in Patients with Myalgic
Encephalomyelitis – Chronic Fatigue Syndrome. 7th International Conference on HHV-6 and 7. March 1, 2011. Reston, VA
4. "Compared to healthy individuals, CFS/ME patients displayed significant increases in IL-10, IFN-g, TNF-a, CD4 + CD25+ T cells, FoxP3 and VPACR2 expression. Cytotoxic activity of NK and CD8+ T cells and NK phenotypes, in particular the CD56 bright NK cells were significantly decreased in CFS/ME patients. Additionally granzyme A and granzyme K expression were reduced while expression levels of perforin were significantly increased in the CFS/ME population relative to the control population. These data suggest significant dysregulation of the immune system in CFS/ME patients."
Immunological abnormalities as potential biomarkers in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis
Ekua W Brenu, Mieke L van Driel, Don R Staines, Kevin J Ashton, Sandra B Ramos, James Keane, Nancy G Klimas, Sonya M Marshall-Gradisnik. Journal of Translational Medicine 2011, 9:81. (2011)
Chronic fatigue syndrome: clinical condition associated with immune activation.Landay AL, Jessop C, Lennette ET, Levy JA. Lancet. 1991 Sep 21;338(8769):707-12.
5. Lapp, Charles W. "Chronic Fatigue is a real disease". North Carolina Family Physician 43:1 (Winter 1992).
Drs.
Cheney and Bell decided in 1988 to mount a collaborative study. They sent blood samples from 104 of their patients to a Los Angeles laboratory. The tests showed that the patients' average interleukin-2 level was 40 times that of healthy control subjects.
6. Campaign for a National ME/CFS Clinic (web site). Listing of Research conducted worldwide section, Immune system dysfunction and abnormalities subsection. Accessed November 2013