Test for Post-Exertional NeuroImmune Exhaustion (PENE) & Post Exercise Malaise, and Muscle Weakness tests.
Scientific and Medical Evidence - Listing of Research conducted worldwide section :
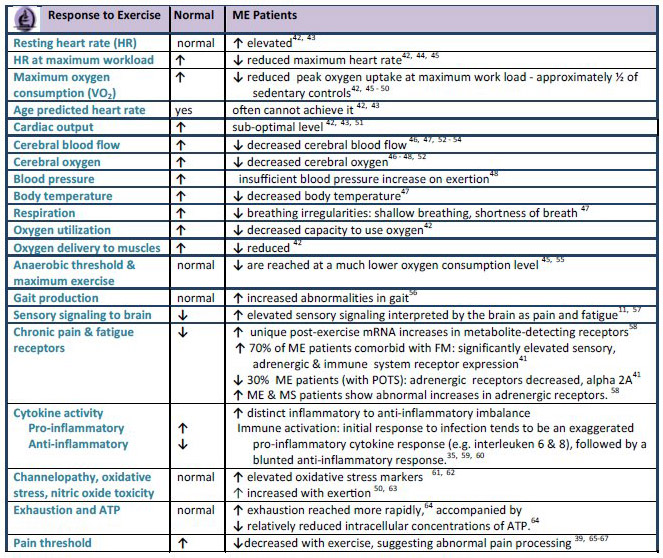
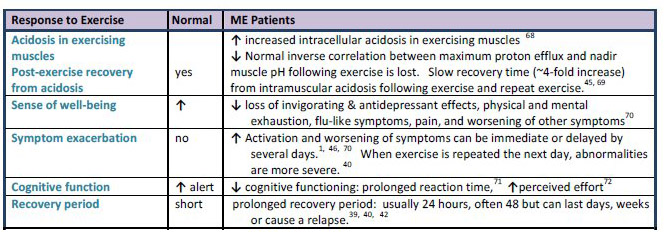
Effects of Exercise
Muscle damage
Cardiac and Vascular and Blood vessel problems. Increased risk of heart attack
Lowered oxygen consumption in ME patients
Increased oxidative stress
Scientific research consistently shows that Post-Exertional NeuroImmune Exhaustion (PENE) is a major factor in ME. The reasons for this are being uncovered by biological and biomedical research worldwide. The research indicates that mitochondria dysfunction, krebs cycle dysfunction, dorsal root dysfunction and accompanying sympathetic nervous system dysfunction, mehtylation cycle and glutathione dysfunction, HPA axis dysfunction, immune system dysfunction and excessive inflammation throughout the body, and cardiac dysfunction are implicated in this.
Tests
Cardiopulmonary exercise testing (CPET) with gas exchange & VO2 Max measurement over two days. The 2 day or 3 day assessment is very important and provides good biomarkers.
- Effects of Exercise
- Symptom exacerbation
- Elevated resting heart rate
- Reduced heart rate at maximum
workload
- Reduced oxygen uptake
- Decreased cerebral blood flow
- Low VO2 max
- Decreased body temperature
- Breathing irregularities
- Gait abnormalities
- Cognitive function/reaction time is
prolonged in post-exertional state
- Increased recovery period
- Pathologically high levels of lactic dehydrogenase, and glutamic oxalo-acetic transaminaser. Dr. Melvin Ramsey
Ramsay A. Epidemic neuromyasthenia: 1955-1978. Postgrad Med J 1978;54:718-21.
- Dr. Christopher Snell (University of the Pacific) recommends cardiopulmonary exercise testing (CPET) with gas exchange as the best way to measure the effects of exercise on ME patients over 2 or more days. This measures several body systems at once.
- Superior Ability of a Two-Day CPET Protocol to Detect Functional Impairment in ME/CFS Compared to Either a Single CPET, A Submaximal Exercise Test, or a VO2 Prediction Equation. Betsy A. Keller, Ithaca College, Dept. of Exercise and Sport Sciences, Ithaca NY
IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
- VanNess JM, Snell CR, Stevens SR, Bateman L, Keller BA. Using serial
cardiopulmonary exercise tests to support a diagnosis of chronic fatigue syndrome.
Med
Sci Sports Exerc
(
2006
)
38
:
S85. doi: 10.1249/000
05768
-
200605001
-
00386.
- Exercise Intolerance: Guide to Management and Treatment. Staci Stevens, M.A., Christopher Snell, Ph.D., Mark VanNess, Ph.D.,
Todd Davenport, DPT
IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
- Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2peak indicates functional impairment. Keller et al. J Transl Med. 2014 Apr 23;12:104.
"ME/CFS patients showed significant decreases from CPET1 to CPET2 in VO₂peak (13.8%), HRpeak (9 bpm), Ve peak (14.7%), and Work@peak (12.5%). Decreases in VT measures included VO₂@VT (15.8%), Ve@VT (7.4%), and Work@VT (21.3%). Peak RER was high (≥1.1) and did not differ between tests, indicating maximum effort by participants during both CPETs. If data from only a single CPET test is used, a standard classification of functional impairment based on VO₂peak or VO @VT results in over-estimation of functional ability for 50% of ME/CFS participants in this study."
- Maureen Hanson (New York,USA) presented research findings on exercise, VO2 and ME at the International ME Conference 2014"CPET using a bike with resistance showed on a 2nd test 24 hours later that CPET values could not be reproduced in ME patients. In other diseases patients can usually reproduce their base response 24 hours later...............ME patients showed a 25% decrease on VO2 max on second day. In patients who also have dysautonomia, the BP does not go up and they have to stop. Subgroups have been detected also in the 2nd CPET, which may correlate with signalling molecules in the blood. There are changes in chemokines and cytokines. 10 cytokines were measured and 5 were decreased markedly. A pilot study compared metabolites in ME patients and found 52 significant differences between before CPET1 and after CPET2. There was reduction in several acylcarnitines after exercise. 300 polar metabolites were examined and 83 differed significantly. Most were higher in controls than patients. Acetyl-carnosine was 2-fold lower in patients than controls.In conclusion: ME patients cannot reproduce their performance on a 2nd CPET. The abnormal responses can affect the autonomic or physiological responses to exercise"
- Vermeulen RC, W VvEI. Decreased oxygen extraction during cardiopulmonary
exercise test in patients with chronic fatigue
syndrome.
J Transl Med
(
2014
)
12
:
20.
- Acidosis (Mitochondria abnormalities in exercised muscles)
Jones DE, Hollingsworth KG, Jakovljevic D
G, Fattakhova G, Pairman J, Blamire AM,
et al. Loss of capacity to recover from acidosis on repeat exercise in chronic fatigue
syndrome: a case
-
control study.
Eur J Clin Invest
(
2012
)
42
:
186
-
194.
- Blood Volume and VO2 max
Farquhar WB, Hunt BE, Taylor JA, Darling SE, Freeman R. Blood volume and its
relation to peak O(2) consumption and physical activity in patients with chronic fatigue.
Am J Physiol Heart Circ Physiol
(
2002
)
282
:
H66
-
H71.
- Some useful information in the following papers
- Balady GJ, Arena R, Sietsema K, Myers J, Coke L, Fletcher GF, et al. Clinician's Guide
to cardiopulmonary exercise testing in adults: a scientific statement from the American
Heart Association.
Ci
rculation
(
2010
)
122
:
191
-
225.
- Bensimhon DR, Leifer ES, Ellis SJ, Fleg JL, Keteyian SJ, Piña IL, et al. Reproducibility
of peak oxygen uptake and other cardiopulmonary exercise testing parameters in
patients with heart failure (f
rom the Heart Failure and A Controlled Trial Investigating
Outcomes of exercise traiNing).
Am J Cardiol
(
2008
)
102
:
712
-
717. doi:
10.1016/j.amjcard.2008.04.047.
75.
- Katch VL, Sady SS, Freedson P. Biological variability in maximum aerobic power.
Med
Sci Sports
Exerc
(
1982
)
14
:
21
-
25. doi: 10.1249/00005768
-
198214010
-
00004.
- Amann M, Subudhi AW, Walker J, Eisenman P, Shultz B, Foster C. An evaluation of
the predictive validity and reliability of ventilatory threshold.
Med Sci Sports Exerc
(
2004
)
36
:
1716
-
1722. doi:
10.1249/01.MSS.0000142305.18543.34
Post Exercise Changes to Genes in ME/CFS
Abnormally changed genes associated with the following biological pathways and proteins after exercise have been linked to CFS according to studies conducted by Dr. Light in the University of Utah, USA:
1. sensory receptors (ASICS, 2PX4, 2PX5, TPRIV1)
2. adrenergic receptors (sympathetic nervous system) (Alpha 2a, Beta-1, Beta-2, COMT)
3. cytokine receptors (IL-6, IL-10, TNF-a, CD14, TLRF4)
There is significant and continuing abnormalities in these genes and receptors after exercise.according to studies conducted by Dr. Light in Utah. See Scientific Evidence Section - Genetic Markers
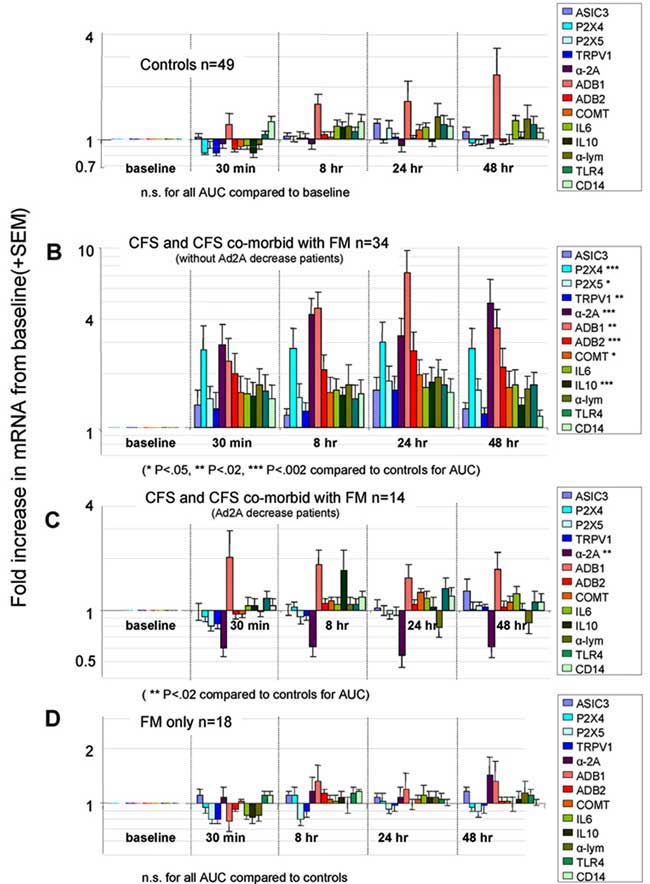
Source: Moderate Exercise Increases Expression for Sensory, Adrenergic, and Immune Genes in Chronic Fatigue Syndrome Patients But Not in Normal Subjects
Alan R. Lightemail address
,
Andrea T. White
,
Ronald W. Hughen
,
Kathleen C. Light. The Journal of Pain
Volume 10, Issue 10 , Pages 1099-1112, October 2009.
Post Exercise Immunological markers
- Elevated levels of RNase L are associated with reduced maximal oxygen consumption (VO2 max) and exercise duration in ME/CFS patients; Snell et al found that both abnormal RNase L activity and low oxygen consumption were observed in most (ME)CFS patients, findings that demonstrate that patients’ extremely low tolerance for physical activity is likely to be linked to abnormal oxidative metabolism, perhaps resulting from defective interferon responses (Comparison of maximal oxygen consumption and RNase L enzyme in patients with CFS. C Snell et al. AACFS Fifth International Research and Clinical Conference, Seattle, January 2001; #026).
- Il1-RA, IL-8, MCP-1 (CCL2) were significantly lower in CFS after one CPET. IL1-RA went down more on day 2 for CFS, and up in controls. Strong indication of immune system dysregulation.
Plasma Cytokines in ME/CFS Patients and Controls Before and After a Cardiopulmonary Exercise Test. Ludovic Giloteaux, Betsy A. Keller, and Maureen R. Hanson.
IACFS/ME Conference. Translating Science into Clinical Care. March 20-23, 2014 • San Francisco, California, USA
Muscle weakness and abnormalties Tests
- Abnormalties in muscle contraction and the covering of muscle fibres which help transmit nerve impulses. Calcium ion transport defects (used for nerve impulses). Defects in blood vessels and in blood circulation to and from the muscles. Oxidative damage to muscle and mitochondria. Dr. Vance Spence
- Abnormalties in the peripheral part of the muscle motor unit using single fibre electromyography. Damage to muscle tissue and muscle fibre as found and described by Dr. Jamal et al.
- Stark T, Walker B, Phillips JK, Fejer R, Beck R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: a systematic review. PM R (2011) 3: 472-479. doi:10.1016/j.pmrj.2010.10.025.
- Wang CY, Olson SL, Protas EJ. Test-retest strength reliability: hand-held dynamometry in community-dwelling elderly fallers. Arch Phys Med Rehabil (2002) 83: 811-815. doi: 10.1053/apmr.2002.32743.
- Andrews AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther (1996) 76: 248-259.
- Van der Ploeg RJO, Fidler V, Oosterhuis HJGH. Hand-held Van der Ploeg RJO, Fidler V, Oosterhuis HJGH. Hand-held myometry: reference values. J Neurol Neurosurg Psychiatry (1991) 54: 244-247.
Post exercise Cognitive tests
- Doctors Jay Goldstein and Ismael Mena (USA), using Zenon SPECT brain scans, demonstrated that the physiological brain function of an M.E. patient rapidly deteriorates after exercise. They also demonstrated that this physiological dysfunction could persist for several days following any of several stressors.
- SeeCognitive Dysfunction Tests section
- VanNess JM, Snell CR, Stevens SR, Stiles TL. Metabolic and neurocognitive responses
to an exercise challenge in chronic fatigue syndrome (CFS).
Med Sci Sports Exerc
(
2007
)
39
:
S445.
- Ocon AJ, Messer Z, Medow M, Stewart J. Increasing orthostatic stress impairs
neurocognitive functioning in chronic fatigue syndrome with postural tachycardia
syndrome.
Clin Sci (Lond)
(
2012
)
122
:
227
-
238.
- Strauss E, Sherman E
MS, Spreen O.
A compendium of neuropsychological tests
. 3rd ed.
New York: Oxford University Press
(
2006
)
.
- Lezak MD, Howieson DB, Loring DW.
Neuropsychological assessment
. 4th ed. New
York: Oxford University Press
(
2004
)
.
- Wechsler D.
Wechsler adult intellig
ence scale
-
revised
.
San Antonio, Texas: The
Psychological Corporation
(
1981
)
Other post exercise abnormalities
The following have been found:
- An oxidative stress study measuring protein carbonyls suggested higher levels of protein oxidation in CFS subjects as opposed to controls.
- Exercise testing in 189 CFS subjects resulted in clinically significant subgroups with 50% of subjects showing moderate to severe functional impairment. An unexpected blunting of Heart Rate and Blood Pressure responses was noted.
- Sarcoplasmic reticulum defect: conduction and calcium transport abnormalities.
- Cardiac muscle—cardiac output found related to illness severity and the predicted exercise-induced relapse.
- Subset of CFS patients with IgM-EBV or CMV-Antibody found to be at risk for cardiac motility abnormalities and occasionally true cardiomyopathy.
- Raises the issue of incomplete viral replication activating immune responses as suggested by Glaser et al.
Sources:
Smirnova IV, “Elevated Levels of Protein Carbonyls in Sera of Chronic Fatigue Syndrome patients,” Mol Cell Biochem Jun 248(1-2) (2003): 93-5.
Vanness JM et al, "Subclassifying Chronic Fatigue Syndrome through Exercise Testing." Med Sci Sports Exerc. Jun 35(6) (2003): 908-913.
Fulle S et al, “Modification of the Functional Capacity of Sarcoplasmic Reticulum Membranes in Patients Suffering from Chronic Fatigue Syndrome,” Neuromuscular Disorders 13 (2003): 479–484.
Peckerman A et al, "Abnormal Impedance Cardiography Predicts Symptom Severity in Chronic Fatigue Syndrome," Am J Med Sci. Aug 326(2) (2003): 55-60.
Lerner AM et al,"Prevalence of Abnormal Cardiac Wall motion in the Cardiomyopathy Associated with Incomplete Multiplication of Epstein-Barr Virus and/or Cytomegalovirus in Patients with Chronic Fatigue Syndrome," In Vivo 18( 4) (2004): 417-424.
Glaser R et al, “Stress-associated Changes in the Steady-state Expression of Latent Epstein–Barr virus: Implications for Chronic Fatigue Syndrome and Cancer,” Brain Behavior and Immunity 19 (2) (2005): 91-103.
Exercise which measures multiple factors
Different types of exercise could be undertaken ranging in intensity and duration. The patient undergoes exercise and the following are measured prior to and after exercise. That is for 3 days after exercise.
- Has mitochondria damage and performance been determined in patient ? have the muscles been checked for this ? what are the effects of exercise on this ?
- Have levels of mitochondria destruction been determined in patient ? have the muscles been checked for this ? what are the effects of exercise on this ?
- Has krebs cycle performance been determined in patient ? have the muscles been checked for this ? what are the effects of exercise on this ?
- Have ADP, AMP, ATP and purine levels been measured ? what is the effect of exercise on these ?
- Has cerebral choline and lactate levels been measures ? what is the effect of exercise on these ?
- Have lactate levels in the blood, muscles and brain been measured ? what are the effects of exercise on this ?
- Has dorsal root function and accompanying sympathetic nervous system functioning level been determined ? what are the effects of exercise on this ?
- Has capacity for metabolite removal from muscle tissues and lactic acid build-up during and after exercise (2-3 days after exercise) been determined in patient ? what are the effects of exercise on this ?
- Has VO2 max been determined for patient ? what are the effects of exercise on this ?
- Has heart rate and HRV been determined ? what are the effects of exercise ?
- Has the effect of exercise on the 2-5a synthetase / RnaseL anti-viral pathway in the immune system and other immune system subsets been determined ?
- Has the effect of inflammatory cytokines and exercise been determined. Does exercise worsen this inflammation ?
- Has methylation cycle performance been determined in patient ? what are the effects of exercise on this ?
- Have glutathione levels been determined in the patient ? have the muscles been checked for this ? what are the effects of exercise on this ?
- Have SOD levels been determined in the patient ? have the muscles been checked for this ? what are the effects of exercise on this ?
- Has HPA axis functioning level been determined for patient ? will cortisol, thyroid hormones, hypothalmic hormones and pituitary hormones be measured ? what are the effects of exercise on this ?
- Has the reticular activating system been determined for patient ? what are the effects of exercise on this ?
- Has cardiac rhythm and cardiac functional analyisis been determined in patient. What are the effects of exercise on this ? if there is a risk of a sudden heart attack, the patient must not start exercise.
- Has blood circulation, including brain blood circulation been determined ? and what are the effects of exercise on this ?
- Has POTS been determined ? and waht are the effects of exercise on this ?
- Has reactive oxygen species and other free radicals levels been measured in patient ? what are the effects of exercise on this ?
- Have inflammatory immune system markers been determined ? what are the effects of exercise on this ?
- Does the patient have an existing viral infection or bacteria, Chlamydia, mycoplasma infection or candida over growth in the intestines ? what are the effects of exercise on this ?
- What genes have previously been identified to be over-expressed by exercise ? what other genes are highly likely to be over-expressed by exercise ? how will this help us understand the structure of causation ?
By monitoring and tracking the above, one can derive objective scientific data regarding Post-Exertional NeuroImmune exhaustion (PENE) and how it's occurring in the patient. This objective data in addition to the patient's own testimony forms the diagnosis of Post-Exertional NeuroImmune exhaustion (PENE).
|