| Damage to the endothelium in blood vessels supplying the brain, spinal cord and nerves
Scientific and Medical Evidence - Listing of Research conducted worldwide section :
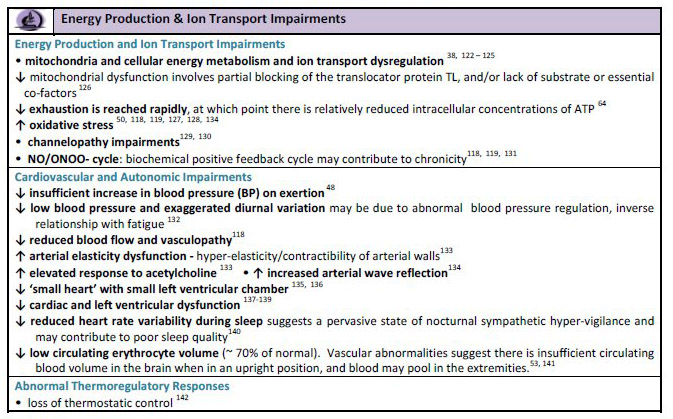
Cardiac
and Vascular and Blood vessel problems. Increased risk of heart attack
Increased
oxidative stress
Substance
P is elevated in ME patients .
Some research studies show damage to the endothelium in blood vessels supplying the brain, spinal cord and nerves in ME patients. This can cause neurological dysfunction. There is also arterial stiffness in many ME patients
Tests
- Flow-mediated dilatation significantly lower. Post-occlusive reactive hyperaemia was also significantly lower. ME patients have significantly higher levels of serum high-sensitivity C-reactive protein and triglycerides and lower levels of serum high-density lipoprotein cholesterol
(Newton DJ, Kennedy G, Chan KKF, Lang CC, Belch JJF, Khan F. Large and small artery endothelial dysfunction in chronic fatigue syndrome. International Journal of Cardiology, 2012 Feb 9; 154(3):335–6 )
- Test for damage to the endothelium in veins and arteries. Test for endothelium dysfunctions.
- Test levels of nitric oxide and endothelin
- Dr. Byron Hyde
- Check for diffuse inflammatory injury of the capillaries at the level of the basement membrane of the brain
- Raynaud's Disease: vasoconstriction, blanching, coldness and pain of extremities.
- Test for defects and dysfunctions of the AV shunts linking veins to arteries. Test for inability to remove wastes from muscles and nerves, and supply oxygen and nutrients to mucles and nerves, and for excessive build up of lactic acid.
- Tests to identify and quantify oxidative damage to the endothelium in blood vessels supplying the brain, spinal cord and nerves. Measure the following: oxLDL (raised in ME) Isoprostanes (raised in ME), GSH (lowered in ME), HDL (lowered in ME), Substance P (raised in ME), c-reactive protein (raised in ME), levels of Homocysteine (raised in ME). Also, measure level of arterial stiffness.
- An enhanced abnormal response or over-sensitivity to ACh.
- Abnormal red blood cell structure and it's effects on micro-circulation. Some scientific studies have found abnormal red blood cell structure in ME patients. The details of this abnormality are outlined in the following research studies.
- L. O. Simpson, 'The Role of Nondisocytic Erythrocytes in the Pathogenesis of Myalgic Encephalomyelitis / Chronic Fatigue Syndrome', The Clinical and Scientific Basis of ME/ CFS [Ottawa, Ontario: The Nightingale Research Foundation, 1992], p. 597
- Mukherjee TM, Smith K, Maros K. Abnormal red-blood-cell morphology in myalgic en-cephalomyelitis. Lancet 1987;2:328-329.20. Simpson LO. Nondiscocytic erythrocytes inmyalgic encephalomyelitis. N Z Med J 1989;102:126-127.21.
- Simpson LO, Murdoch JC, Herbison GP. Red cell shape changes following trigger finger fatigue in subjects with chronic tiredness and healthy controls. N Z Med J 1993;106:104-107
- Infectious Venulitis
Dr. Erich Ryll who is a medical doctor and Professor of Medicine at the University of California, Davis, closely studied Infectious Venulitis since the 1970's and he found many similarities between this illness and ME and CFS. He also studied and examined cases in other countries and found similar results. He believes that a virus is responsible for systemic damage to the body and in particular the vascular system and veins.
Diagnostics - Inflammation of veins, including deep veins. Small haemorrhages around blood vessels in the cerebral cortex extending into the mid-brain, and other areas of the brain. Diffuse micro-haemorrhagic injury of the brain and this occurring around the small blood vessels. Signs of slight vein breakages, minor haemmorhages in different body areas. Easy bruising. Some minor dy-myelination in the brain. Brain hypo-perfusion. Excess pro-inflammatory TH2 cytokines. Difficulty sleeping, unrefreshing sleep. Diffuse pain, headaches, dizziness, brain fog. Poor circulation and feeling cold.
The following articles provide information about this condition
.- Infectious Venulitis, Dr. Erich Ryll
- Simialrities between ME and Infectious Venulitis
- Numerous small haemorrhages around blood vessels in the cerebral cortex extending into the mid-brain (post-mortem of English ME patient Andrew Wallis in 1955)
-
Vasculitis involving the skin was recorded during outbreaks in Cumberland, Durham and North West London in 1955. A maculopapular rash may appear during the return of features of the initial illness such as flu-like symptoms and enlargement of lymph glands and liver.
- Antibody to the muscle tissue in the arterial bed. It is elevated in about 5% of M.E. patients. Dr. Byron Hyde Diagnostic Tests
- Test for Erythrocyte sedimentation rate. The rate is usually very low or zero in ME patients. Canadian clinician Byron Hyde reported in the fall 1989 issue of his newsletter to sufferers, “To my knowledge, there are only five diseases that have a pathological low sedimentation level: myalgic encephalomyelitis (ME also called CFS), sickle-cell anemia, hereditary sperocytosis, hyper-gammaglobulinemia, hyper-fibrogenemia.. Reduced sedimentation rate suggests induced Haemoglobinopathy. (Dr. Paul Cheney)
- Test for mast cell dysfunctions and abnormalities. This is linked to inflammation, pain, and blood vessel abnormalities. Some research findings listed on this link - http://phoenixrising.me/archives/13083 and at this link http://mastcellmaster.com/research.php
Test for:
- Tryptase, histamine, heparin blood
- Eosinophilia, basophilia, monocytosis activity
- Serum chromagranin A
- Serum and urinary leukotriene and prostaglandin isoforms
- Urine methylhistamine after exercise
- Also test for abnormal levels of neuropeptide Y as this directly affects mast cell functions
- Tests to measure neurological dysfunction associated with the above factors
|